



To date, results with at least four models of posterior chamber phakic IOLs of different designs and materials have been discussed in the literature: the Visian ICL (STAAR Surgical),1 the Refractive Implantable Lens (RIL, Appasamy),2 the Eyecryl Phakic IOL (Biotech Vision Care),3 and the Implantable Phakic Contact Lens (IPCL, Care Group).4,5 In this article, we retrospectively report our results with the latest IPCL, the IPCL V2.0, in 74 myopic and myopic-astigmatic eyes treated from April 2018 to January 2020.
PERSONAL EXPERIENCE AND RESULTS
At 3 months postoperative, mean uncorrected distance visual acuity (UDVA) was 1.09 (Snellen decimal scale), mean efficacy index (mean postoperative UDVA/mean preoperative corrected distance visual acuity [CDVA]) was 1.08, and mean safety index (mean postoperative CDVA/mean preoperative CDVA) was 1.24. At 1 year after implantation, mean UDVA was 1.04, even though a toric lens had rotated in one eye.
Average endothelial cell loss between implantation and 3-month follow-up was 1.7% (Figure 1).
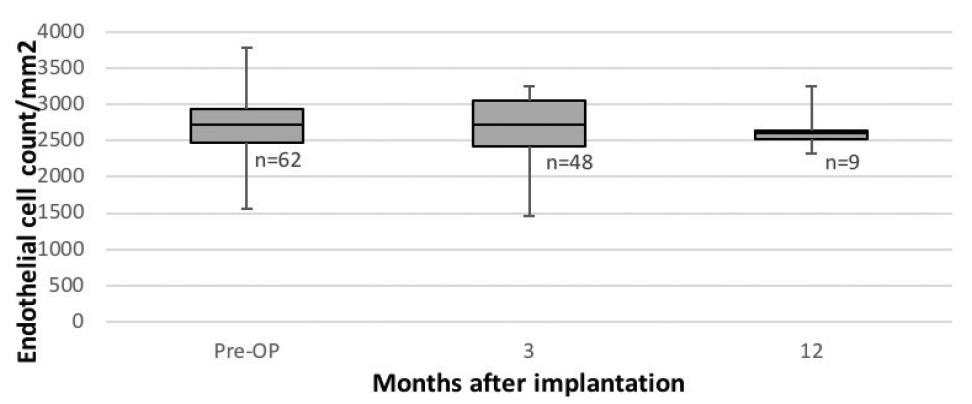
Figure 1. Endothelial cell loss after IPCL implantation over time as measured with noncontact specular microscopy (SP-3000P, Topcon).
Mean IOP was 15.0 ±3.1 mm Hg before implantation. All patients received oral acetazolamide after surgery, and an aqueous release to reduce IOP was performed within a few hours after surgery in six eyes. IOP spikes on the day of implantation were associated with remnants of the OVD used. No glaucoma, uveitis, or any other vision-threatening complication was observed, and at 3 months the average IOP was lower than preoperatively.
We have not yet exchanged an IPCL due to sizing issues. However, additional surgical interventions were performed in five eyes (Table). In one eye (Patient 4 in Table), the toric IPCL had rotated 87° twice without any history of ocular trauma (Figure 2). Of note, the lens vault was within the acceptable range in all eyes at all visits, including the IPCLs that had rotated.
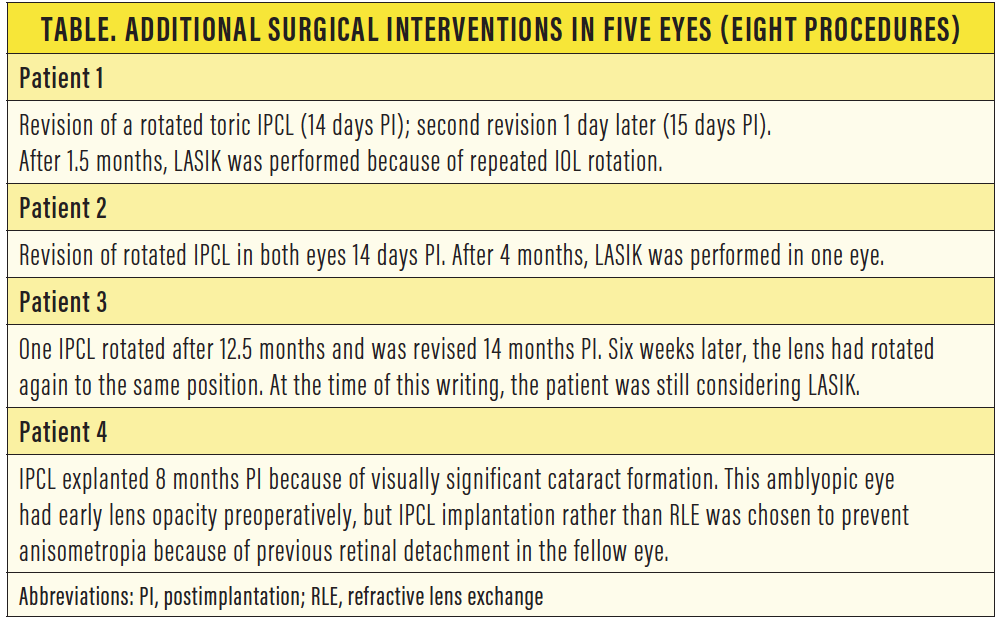

Figure 2. This toric IPCL rotated almost 90° at 12.5 months after implantation.
OFF-LABEL USES
We have used the IPCL off-label in nine eyes in which laser vision correction and refractive lens exchange (RLE) were not preferable options. In five eyes, implantation was classified as off-label because the patient was older than 45 years at the time of surgery. The other four off-label eyes were in two prepresbyopic sisters with bilateral endothelial cell counts of less than 2,000 cells/mm2. Due to their level of accommodative capacity, an RLE was ruled out. The two patients had no signs of ocular pathologies despite very thin corneas, and we are monitoring them closely after implantation.
Postoperative recovery and results have been satisfactory in all off-label uses except for one eye in which an early lens opacity became visually disturbing, necessitating IPCL removal and cataract surgery (Patient 4 in Table).
DISCUSSION
Our initial visual and refractive outcomes and our experience with complications are comparable to our results with the Visian ICL V4c.6 Further, our results validate the findings of Vasavada et al, who reported low surgical and postoperative complications and good visual results at 3 years after IPCL implantation.5
We observed no need for refractive nomogram adjustment when transitioning from the ICL to the IPCL. However, we have performed eight additional surgical interventions after implantation; seven of those were performed because the toric IPCL rotated postoperatively. After the orientation was corrected, most of the rotated IPCLs then rotated back into the same orientation, and we finally treated these patients with LASIK.
The rotation of toric IPCLs was the most important negative issue we experienced. This cannot simply be explained by undersizing of the IPCL because postoperative vaulting was within the acceptable limits of 0.125 to 1.0 mm7 at all postoperative visits, even after rotation. We speculate that individual anatomic factors behind the iris that are not easy to evaluate in a clinical setting might have contributed to this phenomenon.
Endothelial cell loss is a dreaded potential complication after phakic IOL implantation. The physiologic rate of endothelial cell loss is 0.3% to 0.6% per year.8,9 Several studies have shown that, except for the endothelial cell loss related to surgical trauma, annual endothelial cell loss is stable and predictable years after implantation of the ICL.10 It remains to be determined whether this is also true after IPCL implantation. However, reports by Bianchi11 and Vasavada et al,5 like our own short-term results, are promising. Nonetheless, lens manufacturers still recommend regular follow-up after phakic IOL implantation.
The main limitation of our study is its short follow-up period, with only 13 visits at 1 year. Longer follow-up is warranted to determine the long-term stability of visual and refractive results, as well as long-term implications for IOP, endothelial cell loss, and cataract formation.
1. Fernández-Vega-Cueto L, Lisa C, Esteve-Taboada JJ, Montés-Micó R, Alfonso JF. Implantable collamer lens with central hole: 3-year follow-up. Clin Ophthalmol. 2018;12:2015-2029.
2. Pandey S, Sharma V. Commentary: Expanding indications of newer and economically viable phakic posterior chamber intraocular lens designs. Indian J Ophthalmol. 2019;67(7):1066-1067.
3. Yaşa D, Ürdem U, Aǧca A, et al. Early results with a new posterior chamber phakic intraocular lens in patients with high myopia. J Ophthalmol. 2018;2018:1329874.
4. Sachdev G, Ramamurthy D. Long-term safety of posterior chamber implantable phakic contact lens for the correction of myopia. Clin Ophthalmol. 2019;13:137-142.
5. Vasavada V, Srivastava S, Vasavada SA, Sudhalkar A, Vasavada AR, Vasavada VA. Safety and efficacy of a new phakic posterior chamber iol for correction of myopia: 3 years of follow-up. J Refract Surg. 2018;34(12):817-823.
6. Taneri S, Rost A, Hansson C, Kießler S, Dick HB. Klinische Ergebnisse mit zwei phaken Hinterkammerlinsenmodellen zur Korrektur von Myopie und myopem Astigmatismus. Paper presented at: Kongress der DGII; February 13-15, 2020; Mainz, Germany.
7. Instructions for Use. IPCL v2.0; and email communication with Tobias Otte, Polytech Domilens; 2016.
8. Cheng H, Jacobs PM, McPherson K, Noble MJ. Precision of cell density estimates and endothelial cell loss with age. Arch Ophthalmol. 1985;103(10):1478-1481.
9. Jorge J, Queirós A, de Matos SCP, Blasco TF, González-Méijome JM. Age-related changes of corneal endothelium in normal eyes with a non-contact specular microscope. Journal of Emmetropia. 2010;1(3):132-139.
10. Nakamura T, Isogai N, Kojima T, Yoshida Y, Sugiyama Y. Posterior chamber phakic intraocular lens implantation for the correction of myopia and myopic astigmatism: a retrospective 10-year follow-up study. Am J Ophthalmol. 2019;206:1-10.
11. Bianchi GR. Initial results from a new model of posterior chamber implantable phakic contact lens: IPCL V2.0. Med Hypothesis Discov Innov Ophthalmol. 2019;8(2):57-63.
