


Keratoconus is characterized by focal stromal thinning and steepening of the corneal surface. As the disease progresses, it results in the characteristic cone shape of the cornea and causes significant visual impairment. Factors such as aging, diabetes, and tobacco smoking tend to protect against the development of keratoconus. Other factors, including eye rubbing, elevated estrogen, and reduced thyroid hormone action, are associated with keratoconus progression.
Keratoconus tends to progress along the lines of a relapsing-remitting model, in which at some points the disease progresses and at others it goes into remission. This is often due to the aging process, which stiffens the cornea. Other times, the reasons behind converting from a period of stability to one of progression are a mystery. However, we are aware that hormonal changes may predispose some people to develop active keratoconus or ectasia after LASIK and PRK.
One case we published recently adds another item to the hormonal factors that are involved in the development in keratoconus: selective tissue estrogenic activity regulator (STEAR) therapy.1 This article discusses tibolone (Livial, Organon), a STEAR therapy that is available in many countries, including in the European Union. Tibolone is often used in the treatment of endometriosis; it can also be prescribed to postmenopausal women.
PROGRESSION DESPITE AGING
Our report described the case of a 49-year-old woman who had bilateral keratoconus that had been stable for the past 10 years, based on refraction and her corrected distance visual acuity.1 She had been receiving STEAR therapy with tibolone (2.5 mg/day) as a treatment for endometriosis, but around 4 months after initiating STEAR therapy (and 3 months after a bilateral oophorectomy), her keratoconus began to progress again. This case was particularly unusual because aging should have protected against keratoconus progression, especially as the patient was receiving no other systemic or topical mediations other than the tibolone therapy.
Scheimpflug imaging showed changes in corneal topography from pretherapy levels after just 28 days of oral tibolone therapy and bilateral oophorectomy 17 days beforehand. A flattening of the cornea was observed, with maximum keratometry (Kmax) 2.50 D lower in the patient’s left eye than the right. The right eye experienced a flattening of 1.20 D.
Three months later, the patient began to complain about blurred vision in both eyes. Her visual acuity remained 20/20 OD, but it had progressed to 20/50 OS. A steepening of both corneas of up to almost 4.00 D was observed, and Kmax increased by 2.70 D in the right eye and by 3.80 D in the left (Figure 1).
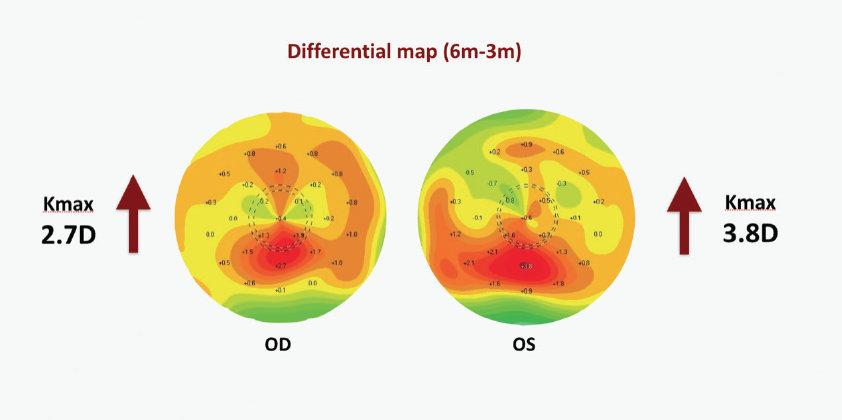
Figure 1. Corneal topographic map showing progression of previously stable keratoconus at approximately 4 months after tibolone therapy was commenced.
CXL WITH MASSIVE FLATTENING
We decided to treat both eyes with epithelium-off accelerated CXL, with an irradiation protocol of 9 mW/cm² for 10 minutes (total fluence, 5.4 J/cm²). At 6 months after bilateral CXL, the right- and left-eye Kmax readings had decreased by 5.50 and 6.10 D, respectively, with 20/16 VA in each eye.
Often, we see a flattening effect of approximately 2.00 D when we perform CXL according to the Dresden protocol, which is currently the most effective protocol for CXL. In our case, however, we saw flattening of up to 6.00 D as long as 9 months after the accelerated CXL protocol (Figure 2).
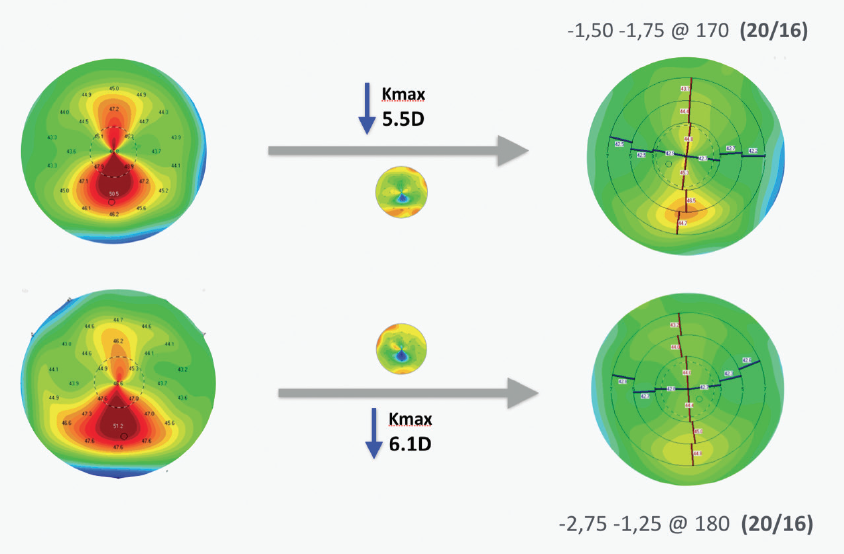
Figure 2. Scheimpflug corneal topography images before tibolone therapy was initiated (left) and the result, 9 months after CXL, of large bilateral flattening (right).
AIMING AT ESTROGEN
What might have caused this? There is a strong similarity between the molecular structure of tibolone and estrogen, as well as two of tibolone’s main metabolites, 3 alpha-hydroxy-tibolone and 3 beta-hydroxy-tibolone. To the best of our knowledge, nothing has been published before about the effects of tibolone in the cornea. Interestingly, it is known that estrogen receptors are present in the corneal stroma, and estrogen receptors are thought to modify the biosynthesis of collagen and glycosaminoglycans—two macromolecules that play a central role in the composition of the cornea and therefore its biomechanics.
There is evidence for estrogen weakening the cornea. Spoerl et al cultured pig corneas in medium with and without beta-estradiol for 7 days and assessed the strength of the corneas through stress-strain analysis.2 They found that corneas cultured with estrogen were on average 36% less stiff than corneas cultured without.
Further, pregnancy has been associated with keratoconus progression in a number of publications from our group.3-5 In 2008, we presented a case in which progression of ectasia occurred during pregnancy despite CXL.3 In 2012, we published a series of patients who demonstrated late onset of ectasia during pregnancy up to 9 years after LASIK surgery.4 In 2013, we reported on transitory variations in keratoconus during pregnancy.5
CONCLUSION
In light of these findings and of our recently published case report, we strongly recommend evaluating the hormonal status of patients with keratoconus or those undergoing refractive laser surgery, including review of medication for endometriosis or following oophorectomy.


