

Since the introduction of laser vision correction (LVC)1 in the form of PRK,2 LASIK,3 or refractive lenticular extraction,4 the stability and persistence of the correction have been a matter of controversy and debate.5 Refractive regression is the term used to describe the loss of the effect of LVC. Regression results in the postoperative refraction deteriorating toward the initial refraction. Although there have been attempts to distinguish topographic/corneal regression (ie, the modified corneal curvature returning toward its preoperative curvature) from refractive progression (ie, the refraction changes due to continued axial length elongation),6 there has been no standardized and universally adopted method to document or study this. Axial length measurement is presently extremely accurate but rarely performed for patients who undergo LVC.
Topographic regression has been often associated with changes in the morphology of the epithelium induced by the alteration in curvature imposed on the underlying change in the stroma as a result of the LVC.7,8
Studies have shown that PRK,9 LASIK,10 and SMILE (Carl Zeiss Meditec)11 are all affected (to different degrees) by the induced epithelial morphological change, most commonly hyperplasia, leading to true topographic regression.
With the advent and refinement of OCT technologies, anterior segment OCT devices have immensely improved the visualization of the corneal epithelium. They have also helped with our understanding of the role the epithelium plays in corneal-induced regression. The device used in the SCHWIND platform is the SCHWIND MS-39,† which incorporates the latest in OCT technology and is combined with the well-established Placido-based topography system (Figure 1). The unique combination makes the SCHWIND MS-39 currently the most advanced diagnostic workstation for corneal work.

Figure 1. The SCHWIND MS-39.
OCT tomographers have a much better resolution and signal-to-noise ratio when compared to Scheimpflug scanning slit tomographers. The SCHWIND MS-39 has unprecedented capabilities in 3D imaging of the epithelial thickness (Figures 2 and 3) without the cumbersome ultrasound water bath system. It is easily comparable to the very high frequency ultrasound system. One of the most important features it has is the ability to measure a widefield epithelial map precisely, easily, and quickly.
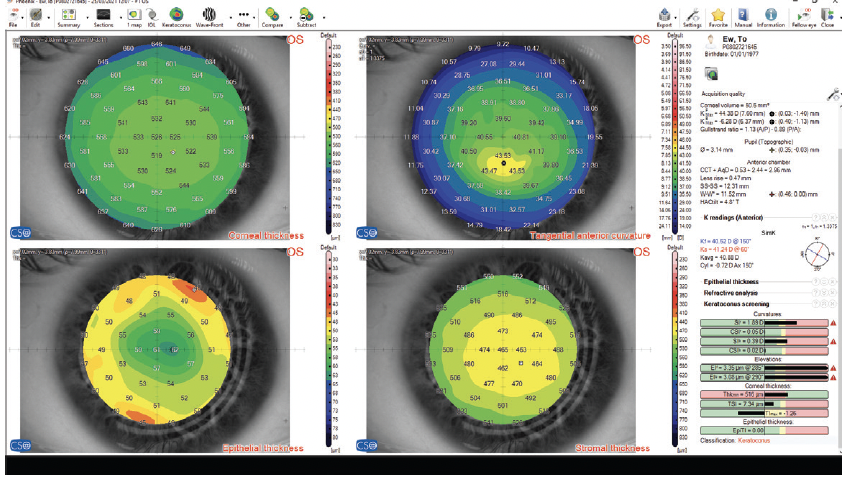
Figure 2. Combination of corneal topography and corneal thickness measurements for both stroma and epithelium.
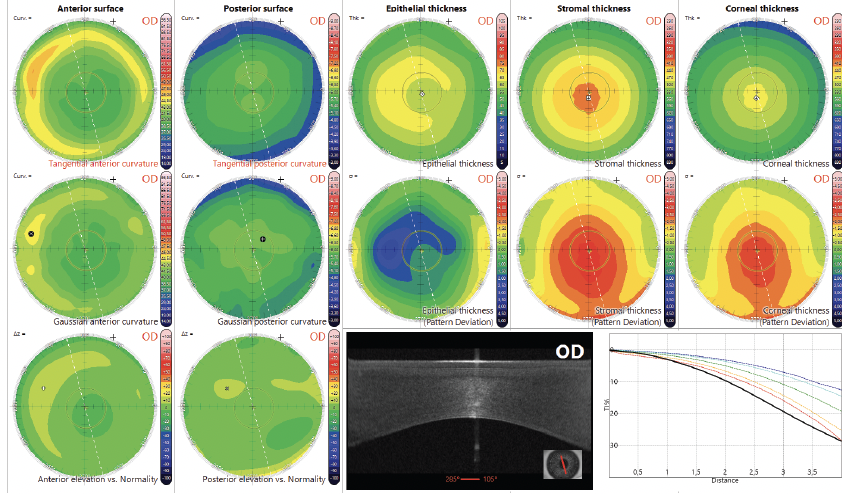
Figure 3. Combination of corneal topography (anterior and posterior cornea) with pattern deviation of corneal stroma and epithelial thickness.
The short- and long-term stability of LVC has been questioned in the past.12 In particular, PRK seems to be associated with an overshoot followed by a reduction of the overcorrection toward the so-called final refraction.13 This has been considered as part of the procedure. It is the weakness of the PRK procedure when compared to LASIK or lenticule extraction with either SMILE or SmartSight (SCHWIND eye-tech-solutions) in which the so-called final refraction is achieved more rapidly.14 It is the same for hyperopic and myopic correction with hyperopic PRK having the longest recovery time.
There are only a few studies trying to distinguish topographic regression from refractive progression.15 Results from these studies show that the epithelium is responsible for short- to mid-term changes at the anterior corneal surface.9 Epithelial hyperplasia can occur in all forms of LVC.16,17
A study of transepithelial PRK (TransPRK) demonstrated essentially no epithelial thickening at 1-month follow-up.18 Another study using the same LVC platform found that thinner corneal epithelium tended to thicken more after TransPRK. Additionally, patients with preoperatively thicker epithelium tended to thin after TransPRK.19
Surface ablation induces corneal surface roughness due to laser spot size and other factors.20-22 This postoperative irregularity elicits an epithelial response that smooths the corneal surface.23 The regrowth of the epithelium compensates for corneal shape modifications. It also lowers the laser-induced irregularities and overall corneal aberrations.24
Huang et al showed that epithelial thickness modulations after ablation can be modeled mathematically to explain clinically observed regression and induction of aberrations.25 A smooth stromal bed26 after the ablation combined with a large optical zone27 and a wide transition zone 28 produces less remodeling of the epithelium. The prophylactic use of CXL has also been proposed to arrest the effects of epithelial remodeling.29
The epithelial refractive power alone is an average of 1.03 D (range, 0.55–1.85 D) over the central 2-mm zone and 0.85 D (range, 0.29–1.60 D) at the 3.6-mm zone.30 Other reports found lower values for the optical power of the epithelium.31
CONCLUSION
The role of the corneal epithelium in the corneal net power and thus total ocular refraction is gaining more importance. The corneal epithelium is one of the final frontiers of LVC surgery. Controlling its thickness, shape, and growth will make LVC more accurate by minimizing the risk of regression.
1. Marshall J, Trokel S, Rothery S, Krueger RR. A comparative study of corneal incisions induced by diamond and steel knives and two ultraviolet radiations from an excimer laser. Br J Ophthalmol. 1986;70(7):482-501.
2. Munnerlyn CR, Koons SJ, Marshall J. Photorefractive keratectomy: a technique for laser refractive surgery. J Cataract Refract Surg. 1988;14(1):46-52.
3. Buratto L, Ferrari M. Excimer laser intrastromal keratomileusis: case reports. J Cataract Refract Surg. 1992;18(1):37-41.
4. Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: all-in-one femtosecond laser refractive surgery. J Cataract Refract Surg. 2011;37(1):127-137.
5. Ficker LA, Bates AK, Steele AD. Excimer laser photorefractive keratectomy for myopia: 12 month follow-up. Eye (Lond). 1993;7(5):617-624.
6. Seiler T, Holschbach A, Derse M, Jean B, Genth U. Complications of myopic photorefractive keratectomy with the excimer laser. Ophthalmology. 1994;101(1):153-160.
7. Lohmann CP, Güell JL. Regression after LASIK for the treatment of myopia: the role of the corneal epithelium. Semin Ophthalmol. 1998;13(2):79-82.
8. Reinstein DZ, Archer TJ, Gobbe M. Rate of change of curvature of the corneal stromal surface drives epithelial compensatory changes and remodeling. J Refract Surg. 2014;30(12):799-802.
9. Sedaghat MR, Momeni-Moghadam H, Gazanchian M, et al. Corneal epithelial thickness mapping after photorefractive keratectomy for myopia. J Refract Surg. 2019;35(10):632-641.
10. Spadea L, Fasciani R, Necozione S, Balestrazzi E. Role of the corneal epithelium in refractive changes following laser in situ keratomileusis for high myopia. J Refract Surg. 2000;16(2):133-139.
11. Reinstein DZ, Archer TJ, Bogge M. Lenticule thickness readout for small incision lenticule extraction compared to artemis three-dimensional very high-frequency digital ultrasound stromal measurements. J Refract Surg. 2014;30(5):304-309.
12. Kato N, Toda I, Hori-Komai Y, Sakai C, Tsubota K. Five-year outcome of LASIK for myopia. Ophthalmology. 2008;115(5):839-844.e2.
13. el-Agha MS, Johnston EW, Bowman RW, Cavanagh HD, McCulley JP. Excimer laser treatment of spherical hyperopia: PRK or LASIK? Trans Am Ophthalmol Soc. 2000;98:59-66; discussion 66-69.
14. Spadea L, Sabetti L, D'Alessandri L, Balestrazzi E. Photorefractive keratectomy and LASIK for the correction of hyperopia: 2-year follow-up. J Refract Surg. 2006;22(2):131-136.
15. Wilson SE, Klyce SD, McDonald MB, Liu JC, Kaufman HE. Changes in corneal topography after excimer laser photorefractive keratectomy for myopia. Ophthalmology. 1991;98(9):1338-1347.
16. Kanellopoulos AJ. Comparison of corneal epithelial remodeling over 2 years in LASIK versus SMILE: a contralateral eye study. Cornea. 2019;38(3):290-296.
17. Ryu IH, Kim BJ, Lee JH, Kim SW. Comparison of corneal epithelial remodeling after femtosecond laser-assisted LASIK and small incision lenticule extraction (SMILE). J Refract Surg. 2017;33(4):250-256.
18. Kaluzny BJ, Szkulmowski M, Bukowska DM, Wojtkowski M. Spectral OCT with speckle contrast reduction for evaluation of the healing process after PRK and transepithelial PRK. Biomed Opt Express. 2014;5(4):1089-1098.
19. Jun I, Kang DSY, Arba-Mosquera S, Kim EK, Seo KY, Kim TI. Clinical outcomes of transepithelial photorefractive keratectomy according to epithelial thickness. J Refract Surg. 2018;34(8):533-540.
20. Netto MV, Mohan RR, Sinha S, Sharma A, Dupps W, Wilson SE. Stromal haze, myo broblasts, and surface irregularity after PRK. Exp Eye Res. 2006;82:788-797.
21. Vinciguerra P, Azzolini M, Airaghi P, Radice P, De Molfetta V. Effect of decreasing surface and interface irregularities af- ter photorefractive keratectomy and laser in situ keratomileusis on optical and functional outcomes. J Refract Surg. 1998;14(2 suppl):S199-S203.
22. Vinciguerra P, Azzolini M, Radice P, Sborgia M, De Molfetta V. A method for examining surface and interface irregularities after photorefractive keratectomy and laser in situ keratomi- leusis: predictor of optical and functional outcomes. J Refract Surg. 1998;14(suppl 2):S204-S206.
23. Fantes FE, Waring GO 3rd. Effect of excimer laser radiant exposure on uniformity of ablated corneal surface. Lasers Surg Med. 1989;9(6):533-542.
24. Reinstein DZ, Archer TJ, Gobbe M. Improved effectiveness of transepithelial PTK versus topography-guided ablation for stromal irregularities masked by epithelial compensation. J Refract Surg. 2013;29(8):526-533.
25. Huang D, Tang M, Shekhar R. Mathematical model of corneal surface smoothing after laser refractive surgery. Am J Ophthalmol. 2003;135:267-278.
26. Aslanides IM, Kymionis GD. Trans advanced surface laser ablation (TransPRK) outcomes using SmartPulseTechnology. Cont Lens Anterior Eye. 2017;40(1):42-46.
27. Kaluzny BJ, Piotrowiak-Slupska I, Kaszuba-Modrzejewska M, Stachura J, Arba-Mosquera S, Verma S. Three-year outcomes after high hyperopia correction using photorefractive keratectomy with a large ablation zone. Br J Ophthalmol. 2019;103(6):849-854.
28. Gauthier-Fournet L, Penin F, Arba Mosquera S. Six-month outcomes after high hyperopia correction using laser-assisted in situ keratomileusis with a large ablation aone. Cornea. 2019;38(9):1147-1153.
29. Kanellopoulos AJ, Asimellis G. Epithelial remodeling after femtosecond laser-assisted high myopic LASIK: comparison of stand-alone with LASIK combined with prophylactic high-fluence cross-linking. Cornea. 2014;33(5):463-469.
30. Simon G, Ren Q, Kervick GN, Parel JM. Optics of the corneal epithelium. Refract Corneal Surg. 1993;9:42-50.
31. Salah-Mabed I, Saad A, Gatinel D. Topography of the corneal epithelium and Bowman layer in low to moderately myopic eyes. J Cataract Refract Surg. 2016;42(8):1190-1197.
†Manufactured by CSO SRL
