
There are more options than ever before for patients who desire correction of their refractive errors. Most recently, intrastromal procedures such as lenticule extraction have become a popular treatment choice for patients because they avoid flap-related complications and reduce the risk of dry eyes after surgery.
We started performing corneal lenticule extraction for advanced refractive correction (CLEAR) with the FEMTO LDV Z8 (Ziemer) in January 2020, just before the COVID-19 pandemic. It took us a little bit of time to gain significant experience with the procedure simply because of the related lockdown and, after our practice reopened, patients’ reluctance to return to their health care providers in the height of the pandemic. Once our surgical volume returned to near-normal levels, however, we saw an increased interest from our patients in the CLEAR procedure.
TWO INCISIONS ARE BETTER THAN ONE
To date, we have performed more than 150 CLEAR procedures. We both had previous experience with lenticule extraction using a different laser platform. The learning curve with the CLEAR technique was therefore straightforward and fast. Regardless of a surgeon’s level of experience with lenticule extraction, one thing that can help shorten the learning curve is creating two guiding tunnel incisions through which the CLEAR procedure can be performed. One incision leads directly into the anterior plane and the other into the posterior plane to ensure the instruments are placed in the correct plane and to decrease the number of manipulations that are required. As you get more confident with the procedure, CLEAR can be performed with just one incision.
In order to build our experience with CLEAR and improve our surgical technique, we scheduled several days in which we would perform between 20 and 40 cases. This helped us to titrate things including the size of the suction ring and the amount of energy applied. Optimizing our settings has helped us to produce superb visual results for our patients. Now, more than 80% of the eyes are 20/25 on day 1 postoperative. That’s very exciting.
From our first cases, we were pleasantly surprised at the simplicity of docking the laser and dissecting the lenticule (Figure 1). To date, neither of us have experienced any complications during dissection such as an incomplete lenticule or suction loss. We also have never had to abort any cases. This is also true for our fellows, who had no prior experience with lenticule extraction. So, in terms of safety, CLEAR is an extremely safe way of performing lenticule extraction.
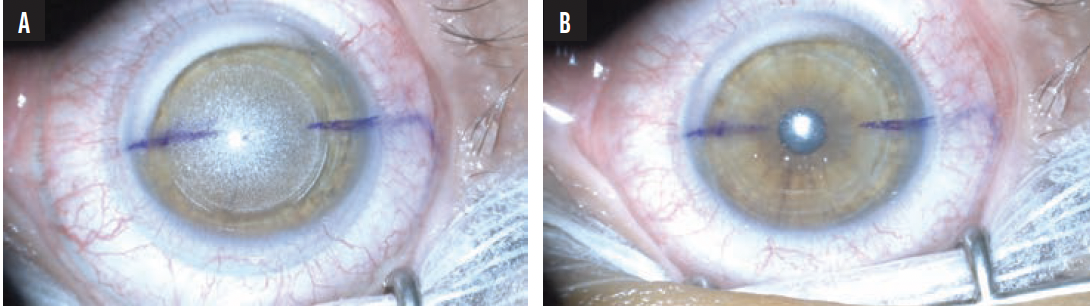
Figure 1. The eye before the lenticule is dissected (A). The eye immediately after the removal of the lenticule (B).
CASE PRESENTATION
A 26-year-old woman presented for a refractive surgery evaluation. She had a manifest refraction of -4.00 -0.50 x 177° OD and -3.00 -0.75 x 7° OS. Her CDVA was 20/20 OU. Preoperative diagnostic imaging is shown in Figure 2. After counseling, the patient decided to undergo CLEAR surgery, and the procedure was scheduled for October 2022.
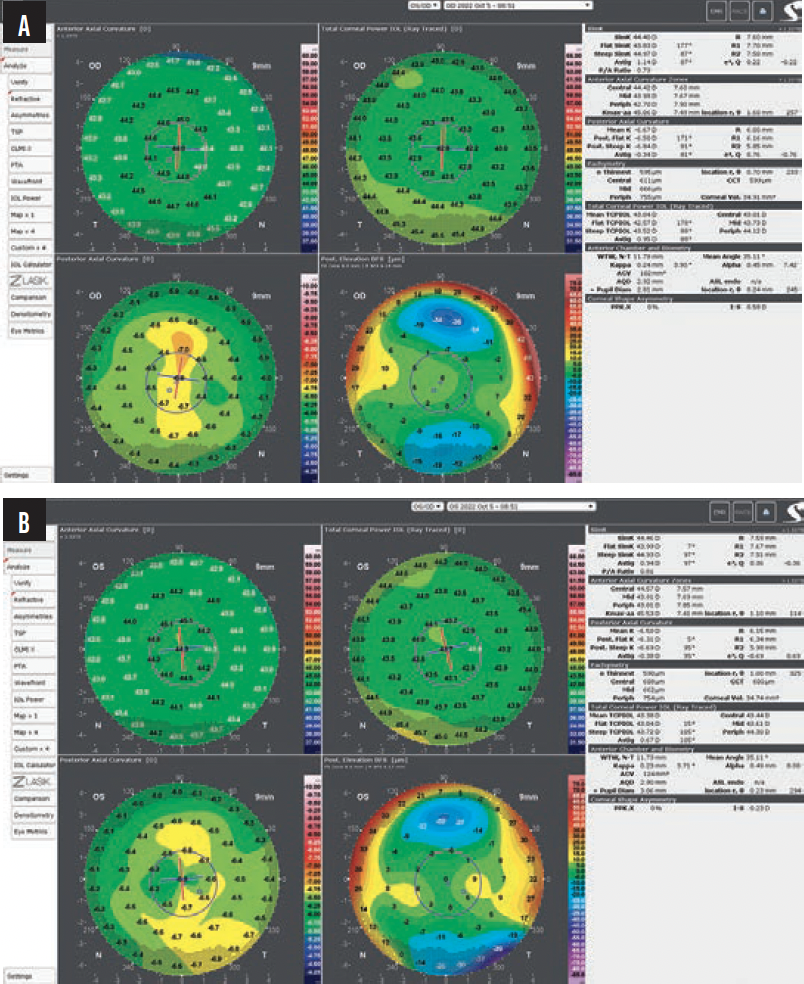
Figure 2. Preoperative corneal topography/tomography (GALILEI) for the right (A) and left (B) eyes.
On postoperative day 1, the patient’s UDVA was 20/25 OD and 20/20 OS with a manifest refraction of 0.00 -0.75 x 8° OD and 0.00 0.00 x 0° OS. CDVA was 20/20 OU. By 1 month postoperative, UDVA had improved to 20/16 OU. The manifest refraction was 0.00 -0.50 x 7° OD and +0.25 0.00 x 0° OS. CDVA further improved to 20/16. The patient was extremely satisfied with her results (Figures 3–5).
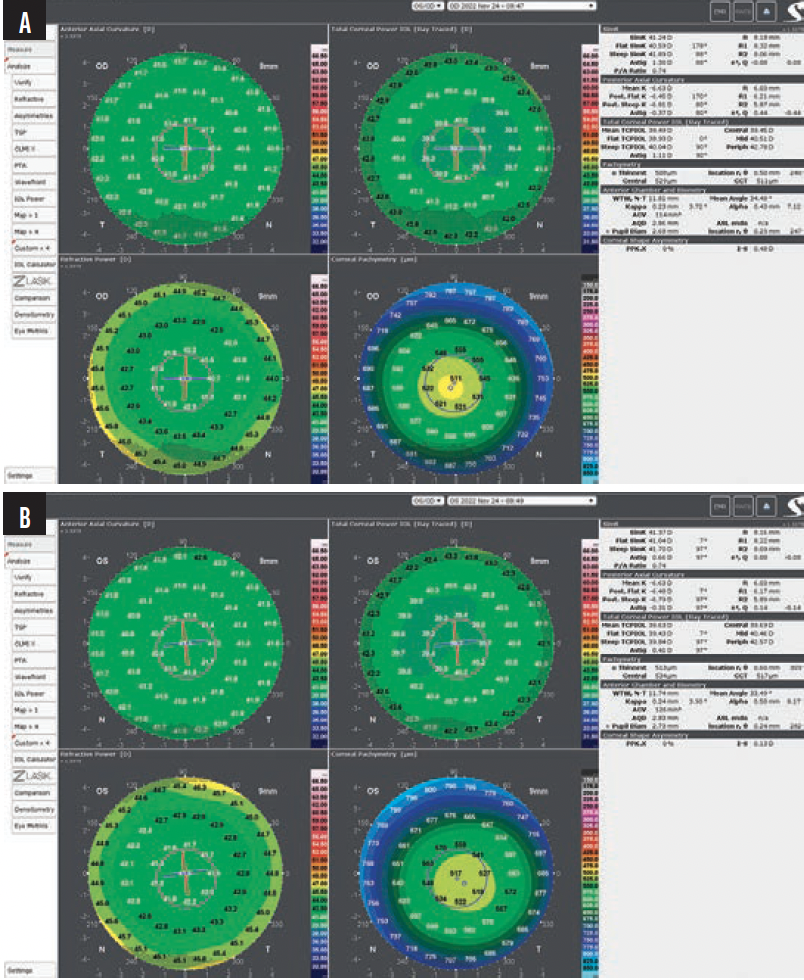
Figure 3. Postoperative corneal topography/tomography (GALILEI) at 1 month for the right (A) and left (B) eyes.
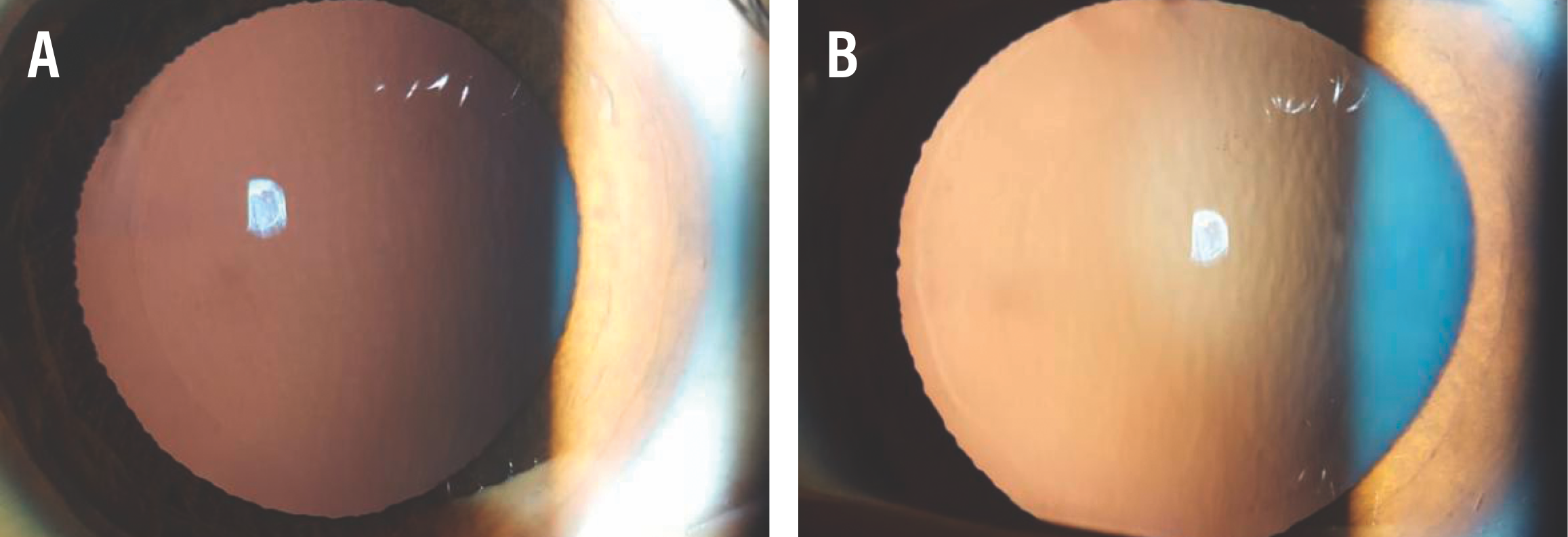
Figure 4. Corneal interface in retroillumination after dilatation at 1 day postoperative for the right (A) and left (B) eyes.
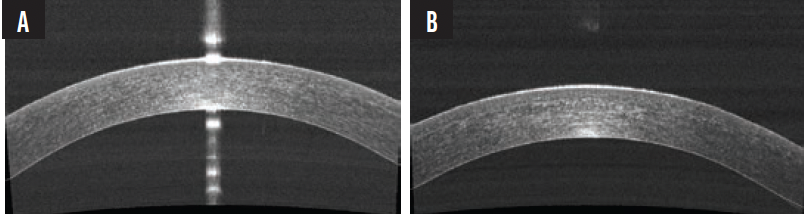
Figure 5. OCT images showing well-apposed, smooth, and regular interfaces at 1 month postoperative for the right (A) and left (B) eyes.
PRACTICE MAKES PERFECT
It can take time to gain comfort and confidence with any new surgical procedure, and CLEAR is no different. It can feel foreign at first to dissect the lenticule, but watching videos and live surgeries and doing wet labs is helpful to hone your technique. The right surgical tools are also essential.
One of the most important early steps of the CLEAR procedure is to make sure that you separate the anterior plane, or the roof of the cap, before dissecting to the bottom. It is also important to perform the dissection 360º to the periphery.
Patient selection is also crucial, especially in early cases. We recommend beginning first with spherical treatments for at least -3.00 to -4.00 D of myopia. In these eyes, the thickness of the lenticule allows easy separation of the planes and extraction. Another helpful tip is to place marks on the cornea to center the treatment to the visual axis and align the axis to compensate for cyclotorsion.
DOCKING
In more than 95% of eyes, we can get good suction and perfect positioning the first time. If needed, the treatment can be easily recentered and the marks on the laser screen can be aligned after docking. This also allows excellent centration and alignment for astigmatism correction.
VISUAL OUTCOMES
Visual rehabilitation after lenticule extraction can be slightly slower than after LASIK. With LASIK, most of our patients are 20/20 on day 1, especially for corrections of -6.00 D or less. With lenticule extraction, day 1 vision might not be as crisp, but by 1 month postoperatively, typically that line of vision is gained and most patients maintain a visual acuity of about 20/20.
Setting expectations is important. When patients understand that their vision might not be crisp on the first day but will get better over time, they are less anxious that something has gone wrong. It is also important to explain the advantages of not having a flap with the CLEAR procedure.
In our opinion, patient selection for CLEAR is similar to that for LASIK. We do not recommend performing CLEAR on eyes with thin corneas and asymmetric astigmatism. For patients who have a little bit of dry eye, it’s possible that lenticule extraction is more suitable than LASIK. The main advantage that we see with CLEAR versus LASIK is that the procedure can be performed through a small incision versus needing to create a large opening of the cornea. This increases the safety of the procedure and can decrease the healing process.
CONCLUSION
CLEAR is an exceptional procedure with proven excellent results. Regardless of your experience level, the learning curve with this technique for lenticule extraction is short. Our residents and fellows have all felt comfortable performing CLEAR within their first few cases.


