
Low-energy laser treatments have many advantages. They maximize precision, minimize tissue damage and the inflammatory response, and aid in fast visual recovery. Corneal lenticule extraction for advanced refractive correction (CLEAR) can be performed with two low-energy laser platforms, the FEMTO LDV Z8 and FEMTO Z8 NEO (both by Ziemer).
I started performing CLEAR more than 3 years ago and continue to be impressed with the results my patients have achieved at every stage of the laser’s development. This article recaps how and why the indications for the CLEAR procedure have expanded over the years and discusses a new bioptics treatment option that combines lenticule extraction with implantation of a phakic IOL.
EXPANDING INDICATIONS
Early in the lenticule extraction procedure’s lifecycle, many surgeons—myself included—positioned the procedure as an option mainly for patients who were contraindicated for other refractive surgery procedures, such as those with high myopia or a thin cornea. Very quickly, however, we started to realize it was advantageous in a larger group of patients other than those in whom we wanted to avoid removing too much corneal tissue.
My very first CLEAR procedure was performed in April 2019. The patient, a 27-year-old man, presented with myopia and blurred vision. There were no significant findings at the slit lamp and no personal history of relevance. The refraction was -5.00 -0.50 x 180º OD. After counseling, the patient decided to undergo CLEAR. On postoperative day 1, UDVA was 20/40 and CDVA was 20/30. At 3 months postoperative, the patient achieved a UDVA of 20/20 and CDVA of 20/20. At his last follow-up, which was at 3 years, the patient’s refraction was stable. He is still very happy with his vision.
Today, my indications for CLEAR have expanded to include patients with higher levels of myopia (-8.00 to -10.00 D) and for patients with astigmatism.
GREAT RESULTS FOR SURGEONS OF ALL EXPERIENCE LEVELS
One of the trickiest parts of performing lenticule extraction is determining if you are in the correct corneal plane. It can be challenging to differentiate between the anterior and posterior surfaces of the cornea.
Compared to other lenticule extraction procedures, both Z8 laser systems can be programmed to create two guiding tunnels, one for the anterior surface and another for the posterior surface of the lenticule, for easy lenticule separation. In other words, the surgeon can program the laser to create two incisions, which is helpful early in the learning curve, or one incision, which surgeons can progress to after gaining experience with and increasing their comfort in the procedure.
The use of two guiding tunnels is preferable in my clinic because we are a teaching institution, and oftentimes our fellows and residents are either observing or assisting in surgery. It is a great way for them to learn CLEAR in a safe and effective way.
A NEW APPROACH TO BIOPTICS
The promising experience I have had with CLEAR over the years has led me to new and exciting treatment possibilities. One of them is combining CLEAR with phakic IOL implantation in a bioptics procedure. Bioptics can be used to address refractive error by combining the use of corneal and lenticular techniques. I believe that it is more precise to correct the cylinder on the cornea versus the lens, and therefore I favor bioptics procedures to the implantation of toric phakic IOLs.
In the past, I performed bioptics by first using LASIK to address the astigmatism and, about 1 month later, implanting a phakic IOL to address the refractive error. Now, however, I perform CLEAR before I implant the phakic IOL. The advantage of using CLEAR instead of LASIK is that it avoids the need for a corneal flap and therefore the risk of flap dislocation during phakic IOL implantation.
CLEAR and phakic IOL implantation are currently staged about 1 month apart, but eventually the hope is that phakic IOL implantation can be performed immediately after the CLEAR procedure. Additionally, it is to be hoped that the combined CLEAR/phakic IOL bioptics procedure can be indicated not for only phakic eyes but also for aphakic eyes.
This is a new concept in bioptics, and at the time this article was written, I had only performed the procedure in five patients. Thus far, however, results have been great and patients are happy with their visual recovery and the quality of their vision (Figures 1-3).
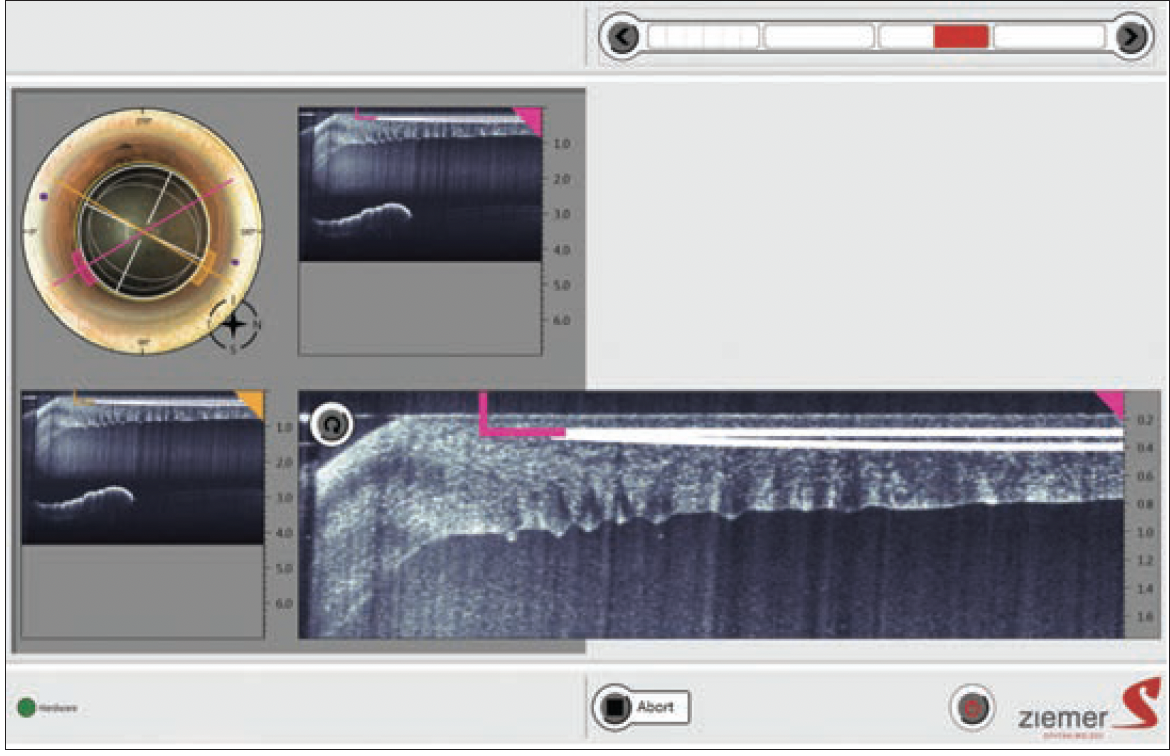
Figure 1. Example of a planned CLEAR/phakic IOL bioptics procedure.
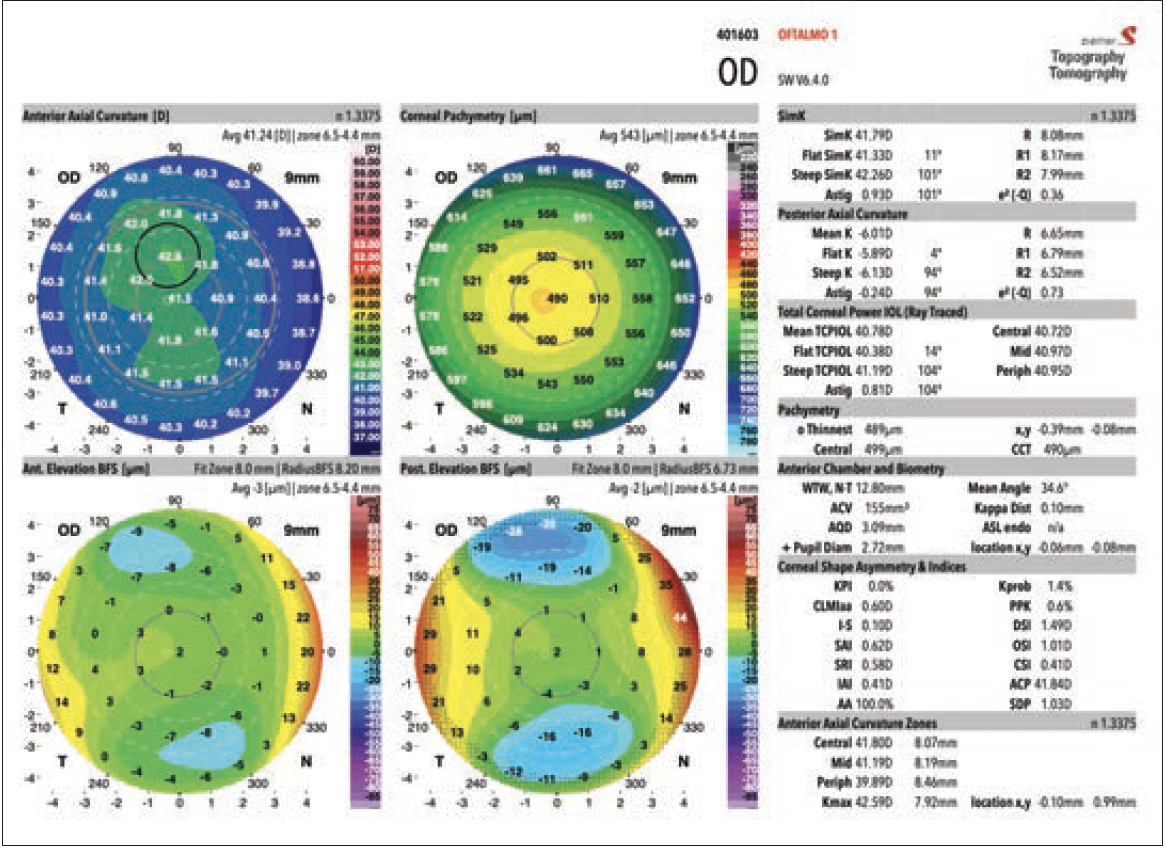
Figure 2. Preoperative corneal topography/tomography (GALILEI).
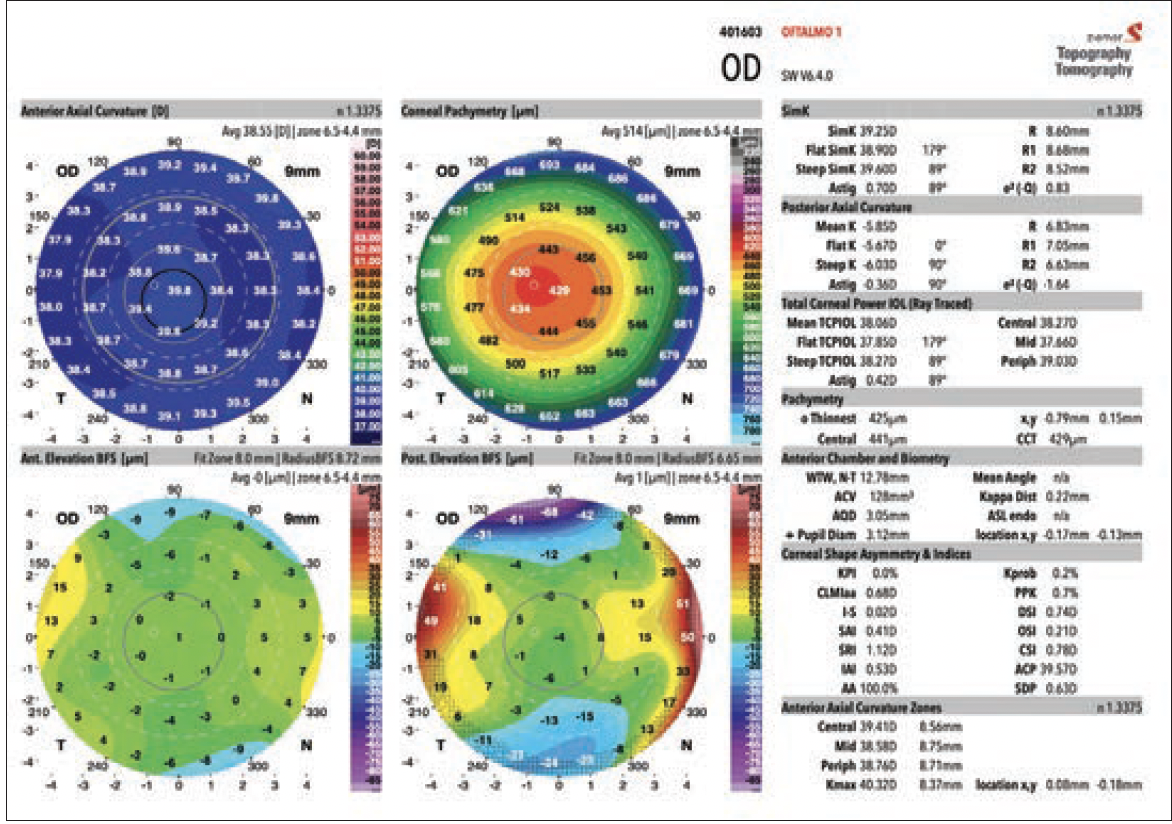
Figure 3. Postoperative corneal topography/tomography (GALILEI).
A VERSATILE LASER PLATFORM
I am a cornea surgeon by nature, and to me the FEMTO LDV Z8 and FEMTO Z8 NEO (Figure 4) are fantastic laser platforms because they are so versatile. In addition to CLEAR, I can use either platform to create pockets for intrastromal corneal ring segments and allograft corneal inlays for keratoconus, as well as for corneal transplants.

Figure 4. FEMTO Z8 NEO and FEMTO LDV Z8.
The intraoperative OCT function is also a useful tool, not only for corneal surgery but also for cataract surgery. I use the Z8 every day for both standard procedures and the new bioptics procedures because it is not only precise but it supports a faster visual recovery and minimal tissue damage and inflammatory response. There is no other laser system that can do what the Z8 platforms can do.

