
INTRODUCTION
Cataract surgery is the most common surgical procedure in the world, and patients generally expect to achieve excellent uncorrected visual acuity and quality of vision. This article shares the viewpoints of two leading surgeons and their early experience with Rayner’s latest enhanced monofocal IOL, RayOne EMV Toric. The surgeons conclude that RayOne EMV Toric is an excellent choice for patients with astigmatism who desire spectacle-free distance and intermediate vision plus functional near vision.
RayOne EMV Toric features a truly nondiffractive optic that provides patients with up to 1.50 D of high-quality vision when targeting emmetropia, together with monofocal levels of contrast sensitivity and dysphotopsia.1-5 To further extend vision, RayOne EMV Toric is optimized for monovision with a unique positive spherical aberration design that provides a smoother transition between distance and near eyes.2,3 The lens is available from 10.00 to 25.00 D in 0.50 D steps and in a wide selection of IOL plane cylinders up to 4.50 D.
Gerd U. Auffarth, MD, PhD, FEBO
Rayner is forging a new path in enhanced monofocal IOLs with its RayOne EMV platform. Both RayOne EMV and RayOne EMV Toric provide patients with an option between standard monofocal and multifocal lenses with diffractive optics.
ADVANTAGES
The lens design and preloaded injector system are both huge advantages of the RayOne EMV IOLs. As a result, there is hardly any learning curve. The nontoric and toric versions can be inserted easily and implanted without much pressure. Further, the anti-vaulting haptic technology provides a very stable platform that doesn’t shift or twist after the lens is implanted. The alignment markings on the RayOne EMV Toric IOL are also highly visible to the surgeon.
The RayOne EMV Toric platform is quite robust against decentration, as well as rotationally stable. With other toric lens designs, a shift of 0.5 to 1 mm can make a huge difference. With RayOne EMV Toric, however, the lens is more forgiving. Additionally, compared to a monofocal toric lens, RayOne EMV Toric provides a better opportunity for patients to achieve spectacle independence, especially with a mini-monovision strategy. Patients routinely achieve excellent distance and intermediate vision and functional near vision.
TECHNIQUE
Especially with advanced technology IOLs, it is paramount to have a round, precisely dimensioned capsule. With RayOne EMV Toric, I prefer a capsulorhexis size between 5 and 5.5 mm. After polishing the capsular bag, I fill it with OVD before injecting the IOL directly into the capsular bag.
The preloaded RayOne injector simplifies insertion. A gentle but consistent pushing of the plunger delivers the first haptic into the capsule, followed by the second. I always rotate the IOL into the final position manually once OVD is removed from the eye.
CONCLUSION
RayOne EMV Toric provides a sharper and wider range of vision compared to monofocal toric IOLs. It is an excellent choice for patients with astigmatism who desire spectacle independence but are contraindicated for multifocal or diffractive (e.g., trifocal) IOLs. The learning curve with RayOne EMV Toric IOL is very short, thanks in part to the lens material and preloaded injector.
CASE PRESENTATION
My first RayOne EMV Toric IOL patient was a 64-year-old woman who presented with subjective deterioration of her vision over the past few months that was worse in the left eye than the right. She reported difficulty driving at night and seeing halos around headlights. Her slit-lamp examination revealed bilateral posterior subcapsular cataracts. She had 1.40 D of astigmatism OD and 1.34 D of astigmatism OS.
IOL calculation with Rayner’s Raytrace Online Premium IOL Calculator (https://rayner.com/en/raytrace/) indicated that a 19.50 D RayOne EMV Toric with 1.50 D of cylinder would be the most appropriate choice for the right eye and a 19.00 D RayOne EMV Toric with 0.75 D of cylinder for the left eye. In the right eye, the IOL was implanted at the 91º axis, and in the left, it was implanted at the 79º axis (Figure 1). After IOL implantation, the toric markings can be seen clearly to be aligned on the respective axis (Figure 1).
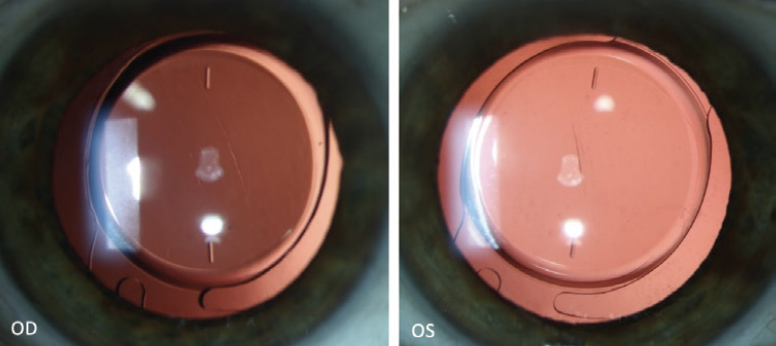
Figure 1. RayOne EMV Toric in the right and left eyes.
At 1 week, the patient’s binocular uncorrected distance visual acuity (UDVA) was -0.20 logMAR, uncorrected intermediate visual acuity (UIVA) at 80 cm was 0.04 logMAR, and uncorrected near visual acuity (UNVA) was 0.20 logMAR with a subjective refraction of plano OD and 0 -0.25 x 100º OS (Figure 2). The binocular defocus curve at 1 week postoperative showed a visual acuity of 0.2 logMAR or better from +1.50 to -2.50 D (Figure 3).

Figure 2. One-week postoperative results with RayOne EMV Toric.
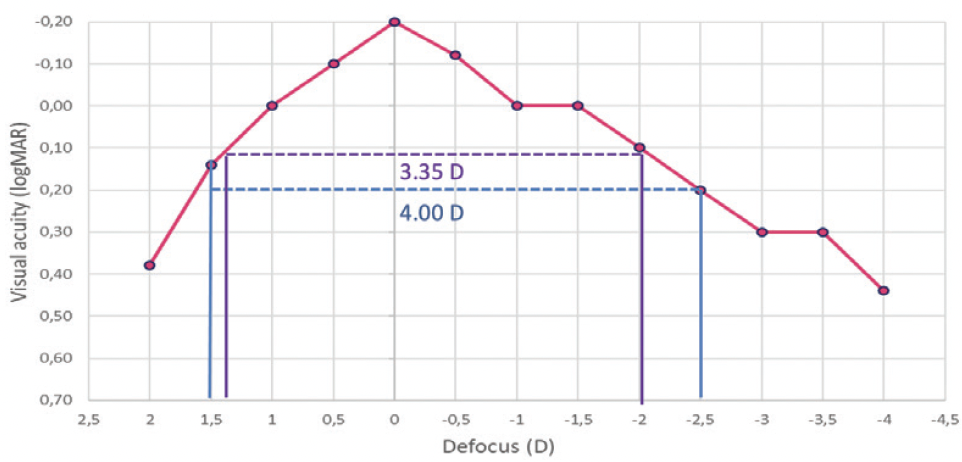
Figure 3. The binocular defocus curve at 1 week postoperative.
The patient reported crisp distance vision and achieved spectacle independence for distance, near, and intermediate. She was extremely satisfied with her results. Halos were not reported postoperatively.
Allon Barsam, MD, MA, FRCOphth
For those patients who have a low tolerance or intolerance of visual disturbances such as halos, RayOne EMV is my go-to IOL. I was the first surgeon in the world to implant RayOne EMV in 2020 and one of the first in the world to implant RayOne EMV Toric in 2022. Both lenses behave like monofocal IOLs, but they also give patients a good amount of intermediate vision. I have found that, when I target slight monovision, patients typically can read unaided. This is a huge upside with the lens.
I like RayOne EMV because it gives patients what I explain to them as natural vision, and, because it has a nondiffractive optic, patients don’t complain of reduced contrast or visual disturbances. I typically target between -0.50 and -1.00 D in the nondominant eye and, in the dominant eye, I select the lens that predicts the lowest positive number or zero.
PERSONAL PREFERENCES
RayOne EMV Toric can be implanted through a 2.2-mm incision, but I prefer to enlarge the incision slightly to ease insertion. I use a wound-assist technique for implantation and my nondominant hand to counter-fixate the eye during insertion. The lens goes easily into the bag, and the anti-vaulting haptic technology ensures that it stays in the bag nicely once the lens is rotated into position. I use the Callisto Eye (Carl Zeiss Meditec) with a 3D heads-up display to align the lens.
CONCLUSION
RayOne EMV reliably provides patients with excellent distance and intermediate vision and functional near vision. There is no additional chair time over a standard monofocal IOL. Now that RayOne EMV Toric gives us the opportunity to eliminate astigmatism at the time of cataract surgery, I find myself implanting this family of lenses in more and more cases.
CASE PRESENTATION
My first RayOne EMV Toric patient was a 56-year-old who presented with a refraction of +4.50 -1.75 x 110º OD and +5.00 -1.50 x 85º OS.
IOL power calculation with the Raytrace Online Premium IOL Calculator indicated that a 24.50 D IOL with 1.50 D of cylinder would be the best option for the right eye. The estimated postoperative refraction indicated a spherical equivalent of plano with +0.10 D of sphere and -0.10 D of cylinder. The IOL was implanted at an axis of 7º (Figure). In his left nondominant eye, we targeted -0.65 D with RayOne EMV because of the minimal corneal astigmatism.
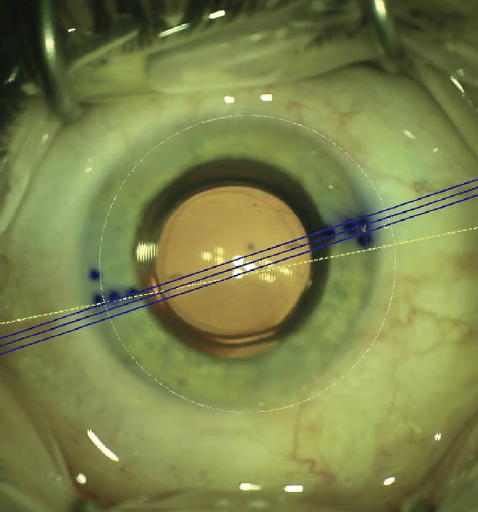
Figure. The RayOne EMV Toric was implanted at the 7º axis.
On postoperative day 1, the patient was very happy with his results. At the 2-week follow-up visit, he achieved 6/6 (20/20) UCVA and was able to see N10 (20/63) at 30 cm and N6 (20/40) at 60 cm. In his left eye, he was able to read N8 (20/50) unaided at 30 cm. Binocular unaided reading vision at 30 cm was N6 (20/40).
1. Ferreira TB. Comparison of visual outcomes of a monofocal, two enhanced monofocals and two extended depth of focus intraocular lenses. Presented at ESCRS 2022; September 16-20, 2022; Milan, Italy.
2. RayOne EMV: First clinical results, Rayner. October 2020.
3. Rayner, data on file.
4. Rayner Peer2Peer webinar. May 2022.
5. Royo M. RayOne EMV and TECNIS Eyhance: A comparative clinical defocus curve. Data on file. 2021.


