
In recent years, technological advancements have transformed cataract surgery into a procedure with advanced refractive goals. In the pursuit of 20/20 or better UCVA, the continuous curvilinear capsulorhexis (CCC) is still widely considered one of the most important steps for generating consistent and predictable outcomes. Regarding IOLs, notable innovations in advanced refractive optics, IOL platforms, and materials have heightened the importance of creating a perfect CCC during cataract surgery.
The ideal anterior capsulotomy is (Figure 1):
- circular and accurately sized between 4.8 and 5.5 mm;
- centered on the patient’s visual axis;1
- able to achieve 360º of symmetrical rim‐to‐optic coverage; and
- capable of producing a strong capsular edge.

Figure 1. An ideal capsulotomy is circular, with 360º of symmetrical rim-to-optic coverage, has a strong edge, and is centered on the visual axis.
In contrast, the consequences of a poorly sized capsulotomy include a malpositioned IOL (e.g., tilt and/or decentration); a potential increase in higher-order aberrations (HOAs); and higher rates of PCO formation (Figure 2).2
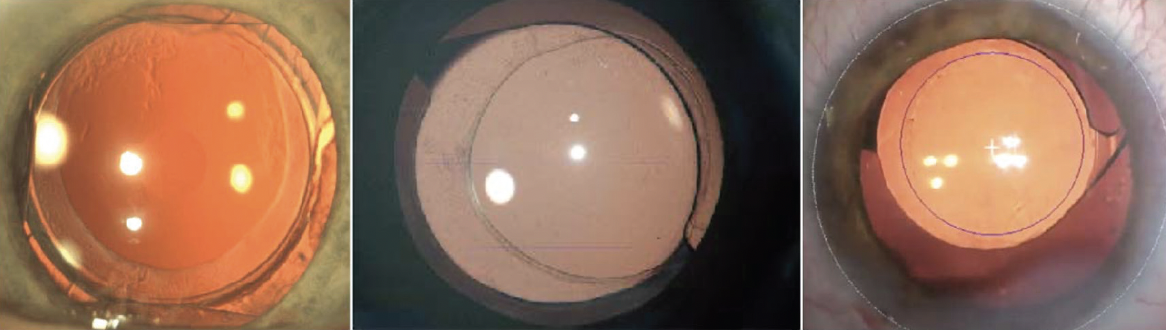
Figure 2. A poorly sized, poorly centered capsulorhexis can cause myriad postoperative complications.
Challenges of a Manual Capsulotomy
Although surgeons can and do achieve reproducible and consistent outcomes with a manual CCC, this requires considerable skill and surgical judgement gained through years of experience. A CCC’s position and shape are influenced by many factors, such as the pupillary dilation, Purkinje images, and the grade of the cataract. To try to improve historical rates of patient dissatisfaction with visual performance and refractive error following cataract surgery, researchers have sought ways to automate the CCC in order to reduce some of the variables from human input.
The Need for Automated CCC Technology
Advancements in IOL optics such as toric, multifocal, and extended depth-of-focus (EDOF) capabilities offer patients increased spectacle independence compared to standard monofocal and enhanced monofocal IOLs, but these premium refractive lenses are very sensitive to alignment, position, and centration. Automating the CCC offers several advantages, including:
- perfect IOL centration with good overlap of the optic rim to stabilize the effective lens position for minimal long-term impact;
- reproducible and repeatable results;
- increased safety in complex cases (e.g., mature & intumescent cataracts, pseudoexfoliation); and
- reduced incidences of PCO.
This article describes several devices that have recently come to market to help surgeons achieve a more reproducible, automated CCC and therefore improve their overall patient outcomes.

FLACS
Femtosecond laser-assisted cataract surgery (FLACS) has challenged the dominance of the manual CCC as the gold standard in cataract surgery. Some studies have demonstrated the improved accuracy of centration, consistency of size, and symmetry of circularity with FLACS.3,4
The strength of the capsulotomy’s edge is particularly important, because a weak edge of a manual CCC has been associated with an increased risk of radial anterior tears.5,6 These tears can extend posteriorly and lead to undesirable complications, and they will negate the possibility of implanting a capsulotomy-fixated lens such as the FEMTIS IOL (Teleon Surgical; Figure 3).

Figure 3. A rendering of the capsule-fixated FEMTIS IOL.
FLACS With the LENSAR ALLY Laser
The ALLY femtosecond laser (LENSAR) is the first second-generation FLACS laser on the market. It employs an Augmented Reality® imaging system and state-of-the-art laser guidance technologies to facilitate FLACS.7 In the treatment planning stage, the ALLY laser scans the relevant structures of the anterior chamber and the lens from six different angles. From these images, and using optical ray tracing techniques, the laser’s Augmented Reality software reconstructs the anterior chamber in 3D and identifies major interfaces such as the anterior and posterior surfaces of the cornea and lens capsule.
Its software determines lens tilt by analyzing the relationship of the anterior and posterior curvatures of the lens capsule to the optical axis. With this information, the ALLY laser can center the anterior capsulotomy symmetrically over the optical axis (or pupil’s center). To make the arcuate incisions, it aligns intraoperative imaging with preoperative corneal biometry, and it performs iris registration to compensate for cyclotorsion. A low-pressure liquid interface enables the capsulotomy’s construction with no compression of the cornea, while the laser makes imaging adjustments in real time for the most accurate corneal incisions. The result is a 100% circular, free-floating capsulotomy. To fragment a cataractous lens, the ALLY can define the grade of cataract intraoperatively and then apply preloaded fragmentation patterns for any cataract density with precise spot application.
For astigmatic eyes, the ALLY laser offers the IntelliAxis Refractive Capsulorhexis® toric IOL alignment, which uses small tabs superimposed on the capsular rim to indicate the intended axis, both intra- and postoperatively. Additionally, the laser’s Streamline® technology provides precise arcuate incisions.
Zepto® Precision Pulse Capsulotomy
Approved by the FDA in 2017, the Zepto Precision Pulse Capsulotomy (PPC; Centricity Vision) consists of a small console (ZeptoLink) that connects to a disposable handpiece with a low‐profile, transparent silicone suction shell. Inside the eye, the clear suction shell creates a 360° apposition with the surface of the anterior capsule via a flexible nitinol ring. The ring delivers a series of rapid thermoelectric nanopulses to cleave 360º of the anterior capsule in <5 msec.
Early clinical experience with the Zepto device has shown consistent results, with potential value for complex cases such as in eyes with small pupils, zonulopathy, or intumescent or brunescent lenses.8,9 However, reports of radial tears and incomplete capsulotomies have prompted improvements and modifications, and there may be a learning curve. Additional studies are warranted to further evaluate PPC with Zepto.
CAPSULaser Selective Laser Capsulotomy
The CAPSULaser (Excel‐Lens, Inc.) is a class 4 solid-state, continuous-wave laser that performs a selective laser capsulotomy (SLC). The device is portable and affixes to the binocular indirect connection points of any operating microscope, and then delivers thermal energy to create a circular capsulotomy in less than 1/3 of a second. Surgeons usually stain the anterior capsule with an enhanced solution of trypan blue dye to give the laser a target. The laser projects a reticule as a guide for the surgeon to follow for centration, which is adjustable from 4.5 to 7 mm in diameter.
In addition to advantages related to efficiency, Daya et al demonstrated that this SLC technique may provide a more stabilized and strengthened anterior capsule compared to manual CCC and FLACS.10 However, CAPSULaser cannot fragment a lens or create incisions; it is only used for auto-CCC creation.
Conclusion
Surgeons continue to seek reliable means for creating reproducible capsulotomies that can optimize outcomes without sacrificing time or efficiency. Notable innovation has occurred in this space, including a trend toward guided or automated approaches for improved reproducibility and precision, particularly for eyes receiving capsulorhexis-fixed advanced-optics IOLs. With time, more comparative studies with automated capsulotomies will help us surgeons evaluate their performance and determine whether their improved geometry translates to meaningful benefits for our patients.
1. Okada M, Hersh D, Paul E, van der Straaten D. Effect of centration and circularity of manual capsulorrhexis on cataract surgery refractive outcomes. Ophthalmology. 2014;121(3):763-770.
2. Gu X, Chen X, Jin G, et al. Early-onset posterior capsule opacification: incidence, severity, and risk factors. Ophthalmol Ther. 2022 Feb;11(1):113-123.
3. Tackman RN, Kuri JV, Nichamin LD, Edwards K. Anterior capsulotomy with an ultrashort-pulse laser. J Cataract Refract Surg. 2011;37(5):819-824.
4. Verdina T, Peppoloni C, Barbieri L, et al. Long-term evaluation of capsulotomy shape and posterior capsule opacification after low-energy bimanual femtosecond laser-assisted cataract surgery. J Ophthalmol. 2020:6431314. eCollection 2020.
5. Friedman NJ, Palanker DV, Schuele G, et al. Femtosecond laser capsulotomy. Cataract Refract Surg. 2011;37(7):1189-1198.
6. Mastropasqua L, Toto L, Mattei PA, et al. Optical coherence tomography and 3-dimensional confocal structured imaging system-guided femtosecond laser capsulotomy versus manual continuous curvilinear capsulorhexis. J Cataract Refract Surg. 2014;40(12):2035-2043.
7. Packer M, Klyce SD, Smith C. The LENSAR® Laser System–fs 3D for femtosecond cataract surgery. Available at: https://lls.lensar.com/wp-content/uploads/2021/07/LENSAR-Overview-White-Paper.pdf. Accessed June 11, 2024.
8. Chang DF, Mamalis N, Werner L. Precision pulse capsulotomy: preclinical safety and performance of a new capsulotomy technology. Ophthalmology. 2016;123(2):255-264.
9. Chang DF. Zepto precision pulse capsulotomy: A new automated and disposable capsulotomy technology. Indian J Ophthalmol. 2017;65(12):1411-1414.
10. Daya S, Chee S-P, Ti S-E, Packard R, Mordaunt DH. Comparison of anterior capsulotomy techniques: continuous curvilinear capsulorhexis, femtosecond laser-assisted capsulotomy and selective laser capsulotomy. Br J Ophthlmol. 2020;104(3):437-442.

