

Over the past decade, the term refractive cataract surgery has become more commonly used to describe cataract surgery. This terminology, in large part, is due to the accuracy of refractive outcomes that we can now provide our patients after surgery.
Although many elements are involved in the practice of refractive cataract surgery, one of the most crucial is the ability to calculate IOL power effectively and efficiently.
battling refractive surprises
Historically, surgeons have relied on formulas such as the Hoffer, Holladay, and SRK-T, and, more recently, on the Olsen and Barrett Universal II, to calculate IOL power. Each has added incrementally to our overall accuracy, yet we still have refractive surprises that fall short of our patients’ and of our expectations.
Even as the formulas parse the variables involved in vergence calculations of the expected lens position into smaller subsets of patient cohorts, within each subset a regression still exists with data to either side of a regression line.
Another new alternative, the Hill-RBF calculator, selects IOL power using artificial intelligence–driven pattern recognition. Available on the Lenstar (Haag-Streit), this new data-driven method to determine IOL power does not depend on effective lens position and does not have any calculation bias. The basis of the Hill-RBF calculator is described in the previous article by Warren E. Hill, MD, and below I provide a general history of IOL power calculation and further focus on the clinical outcomes with this new method of IOL power calculation.
OLD VersuS NEW
In the very early days of IOLs, before the emergence of accurate biometry, lens power was selected solely based on type of refractive error: rules of thumb assigned average eyes to a 21.00 D lens, myopic eyes a 15.00 D lens, and hyperopic eyes a 25.00 D lens, with gross interpolations based on refractions.
Then, in the 1980s, regression formulas surfaced, helping to incrementally increase the predictability of refractive outcomes after cataract surgery. These empiric formulas were generated by retrospectively analyzing and averaging data from a large number of patients who had undergone cataract surgery. Although the use of regression formulas provided better means of refractive prediction than simply correlating IOL power to the type of refractive error, lens power errors were commonplace.
The development of better diagnostic technologies to measure parameters such as anterior chamber depth, keratometry, and axial length then allowed cataract surgeons to use more precise mathematical formulas to calculate IOL power. Today, theoretical formulas such as SRK-T, Holladay 1 and 2, Hoffer-Q, Haigis, Olsen, and Barrett Universal II are rooted in geometrical optics. However, because they require an estimation of the lens position (ie, effective lens position), refractive errors can still occur postoperatively. Additionally, whereas increasingly sophisticated IOL power calculation formulas can get closer to its goal by adding more data (eyes), there still will be points that are above and below the line.
a league of its own
The above is not true for the Hill-RBF calculator, which looks at each data point (eye) independently, as it exists relative to outcomes from its fellow data points (eyes). The reason that the Hill-RBF calculator is so fundamentally different from theoretical IOL power calculation formulas is this: The more eyes that are added to the database, the higher the likelihood that similar eyes are available and the more accurate the calculator becomes.
Additionally, the Hill-RBF calculator can determine if it does not have enough data to make a good estimation of IOL power. In simpler terms, it tells you when it is likely to be right and when it is not sure. From a clinical perspective, that is great, as there is nothing I like more than knowing what my level of confidence in a piece of information should be.
EARLY EXPERIENCE
I have been using the Hill-RBF calculator since January 2016. I was privileged to be part of the initial multicenter prospective study, conducted across three sites, to test the beta version of the calculator. In 459 eyes scheduled for cataract surgery, IOL power was calculated based on the legacy formulas and on the Hill-RBF beta calculator, which included data points from the initial 3,400 eyes used to train the artificial intelligence program. We then looked at patients’ 1-month final refractions in order to determine how well the Hill-RBF calculator compared with the IOL power calculation formulas.
What we found was that the Hill-RBF calculator outperformed all of the selected formulas in long eyes (Figure 1), in average eyes, and in short eyes. Using the benchmark of ±0.50 D target spherical equivalent, 91% of all eyes that were considered in-bounds by the calculator—that is, all preoperative measurements resided within the six pair-wise boundary models—were within this range (Figure 2). An out-of-bounds calculation, on the other hand, was defined as any preoperative measurement that resided outside just one of the pair-wise boundary models (Figures 3 and 4). This occurred in a very low percentage of eyes.
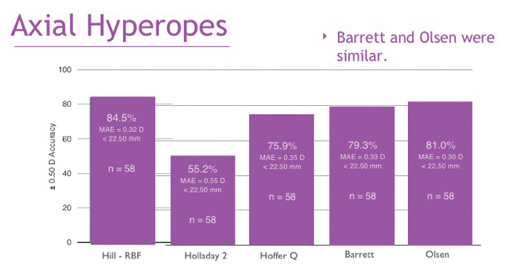
Figure 1. The Hill-RBF calculator compared with other IOL power calculation formulas in long eyes.
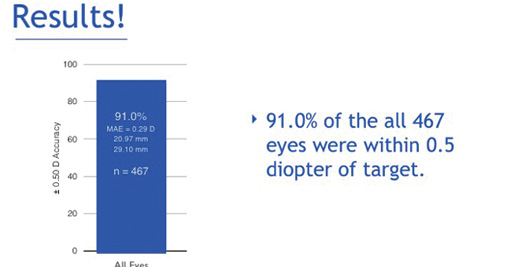
Figure 2. The percentage of eyes within ±0.50 D target spherical equivalent with the Hill-RBF calculator.
Considering that more than 3 million cataract surgeries are performed yearly in the United States alone, 3,400 eyes is a small data set. We can postulate that, as data from more eyes are imported into the calculator, its preciseness will continue to increase.
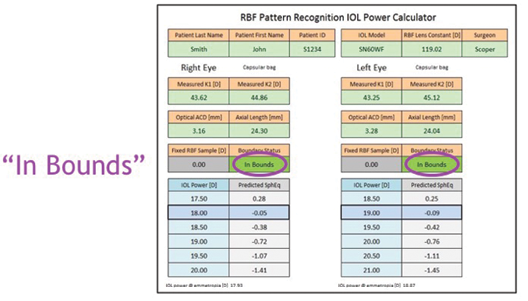
Figure 3. An in-bounds calculation with the Hill-RBF calculator.
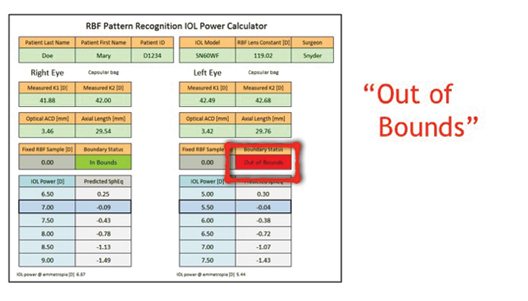
Figure 4. An out-of-bounds calculation with the Hill-RBF calculator.
GOOD NEWS FOR PATIENTS
A lot of the IOL power calculation formulas in use today harken to the pre-millenium change era in which they had been held to a standard of ±1.00 D target spherical equivalent; however, with patient expectations after cataract surgery being so high, we really need to be within ±0.50 D to meet the refractive outcomes required of spectacle independence, especially with premium IOLs. The Hill-RBF calculator could very well be the best tool to get us within this range.
Personally, ever since the data from the prospective study was analyzed, I have been using the Hill-RBF calculator exclusively for eyes in which it provided an in-bound result. In these approximate 1,000 cases, the postoperative refractive results have been phenomenal. I have not crunched the exact numbers since the prospective study closed, but, if I had to guess, only a low single-digit percentage of eyes returned an out-of-bounds result.
Given that the prospective study was conducted using the highest standard of target spherical equivalent (±0.50 D) and that the Hill-RBF calculator outperformed several sophisticated IOL power calculation formulas in every category, it is safe to say that the Hill-RBF calculator has the potential to further enhance refractive outcomes beyond even high levels of success that we and our patients enjoy today.
