

Just like Béatrice Cochener, MD, PhD, has indicated in the previous article, the excellent outcomes I have had with the FineVision trifocal IOL (PhysIOL) have extended to the latest iteration of this lens, the FineVisionHP. In my article, I will discuss the first clinical outcomes with this new hydrophobic trifocal lens and compare those results to the results with a hydrophilic trifocal lens.
STUDY DESIGN
We carried out the prospective, randomized, controlled study of the FineVision trifocal and the FineVisionHP trifocal at Semmelweis University in Budapest, Hungary. Built on the same platform and optical design, the main difference between the lenses is that the former is a hydrophilic and the latter a hydrophobic. Additionally, the FineVisionHP is made of a glistening-free material (G-free) and incorporates RidgeTech technology, which helps to decrease the stickiness of the hydrophobic haptics.
Inclusion criteria were cataract formation with no other eye comorbidity, at least 50 years of age, regular corneal astigmatism less than 0.75 D, a desire for spectacle independence, and realistic expectations. As we all have seen in our practices, more and more presbyopic patients with a clear lens are searching for a solution to their visual symptoms; they want very good vision and very well-predicted results. The FineVisionHP is a wonderful choice for these patients as well, but they were not included in this study. The exclusion criteria were unrealistic expectations, irregular or high regular corneal astigmatism, any other ocular comorbidity, a history of ocular trauma or prior ocular surgery including refractive procedures, capsule or zonular abnormalities, and pupil abnormalities.
A total of 25 mainly hyperopic and presbyopic patients (50 eyes) were enrolled in the study. Among them were 15 women and 10 men, and their average age was 58.8 years. In each case, the patient received the hydrophilic FineVision IOL in one eye and the hydrophobic FineVisionHP IOL in the other. There was no statistically significant difference in the subjective refraction, corneal astigmatism, IOP, axial length, and anterior chamber depth between the eyes of each individual.
The IOL power calculation was performed by the Lenstar (Haag-Streit) using one of the following formulas: SRK/T, Hoffer Q, Holladay 1, and Haigis. The target refraction was planned slightly hyperopic in the dominant eye and slightly myopic in the nondominant. The spherical diopter of the IOLs was similar, around 22.00 D.
FOLLOW-UP AND RESULTS
Follow-up. Patients reported for postoperative follow-up on days 1, 3, and 6 and at 6 months. At each visit, we checked the visual acuity with the ETDRS chart using near, intermediate, and distance targets of 35 cm, 70 cm, and 4 m, respectively, under both photopic and mesopic conditions. We also tested the contrast sensitivity under both conditions. Table 1 shows the pre- and perioperative data with the hydrophilic and the hydrophobic FineVision lenses.
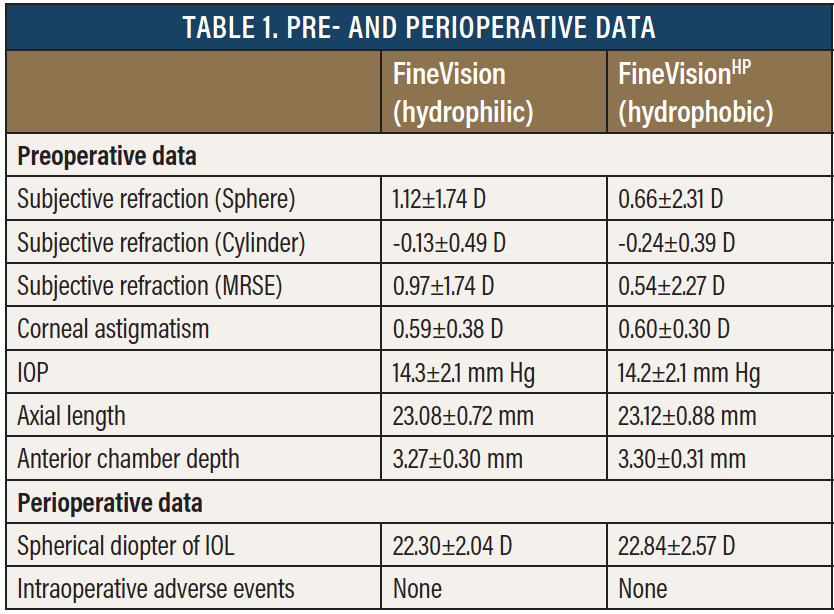
Results. There were no intraoperative adverse events. The manifest refractive spherical equivalent with the hydrophilic and hydrophobic lenses, during the first 6 months of follow-up, was about 0, and this is quite a nice result. The BDVA and the UDVA also ran parallel with the two types of lenses (Figure 1), which was about 0 logMAR. Likewise, the DCNVA and UNVA (Figure 2) and the DCIVA and the UIVA (Figure 3) between the two IOLs were similar. There was no statistically significant differences between the two study groups in any of these categories.
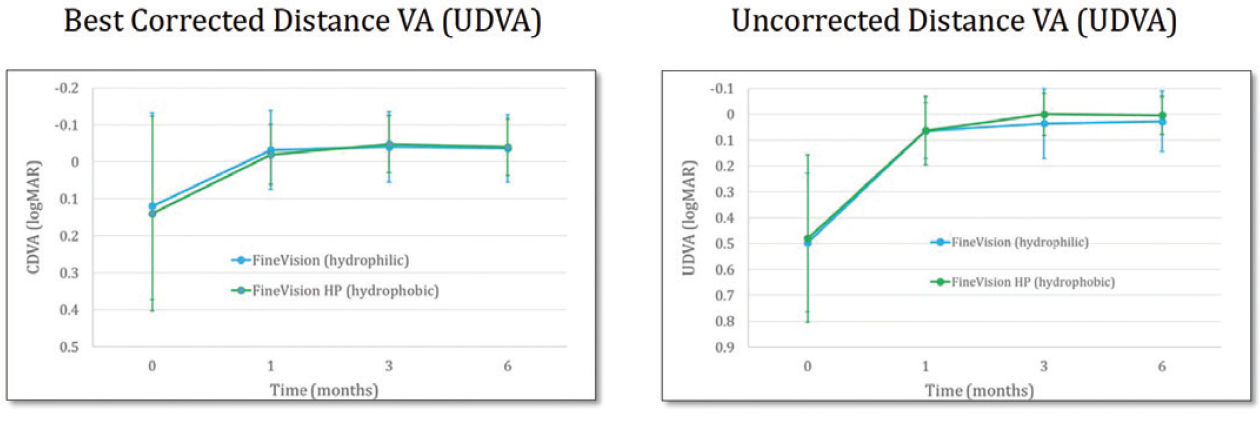
Figure 1. Distance visual acuity with the FineVision and FineVisionHP lenses.
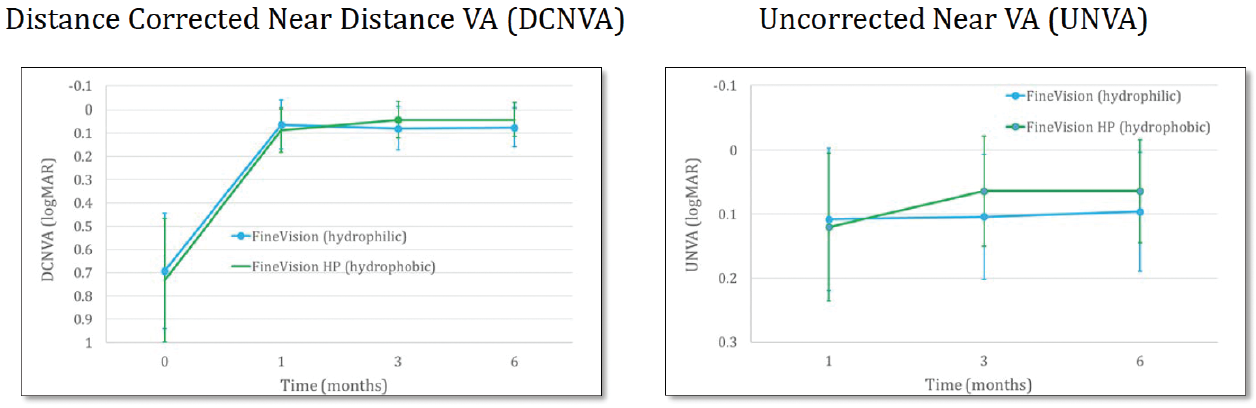
Figure 2. Near visual acuity with the FineVision and FineVisionHP lenses.
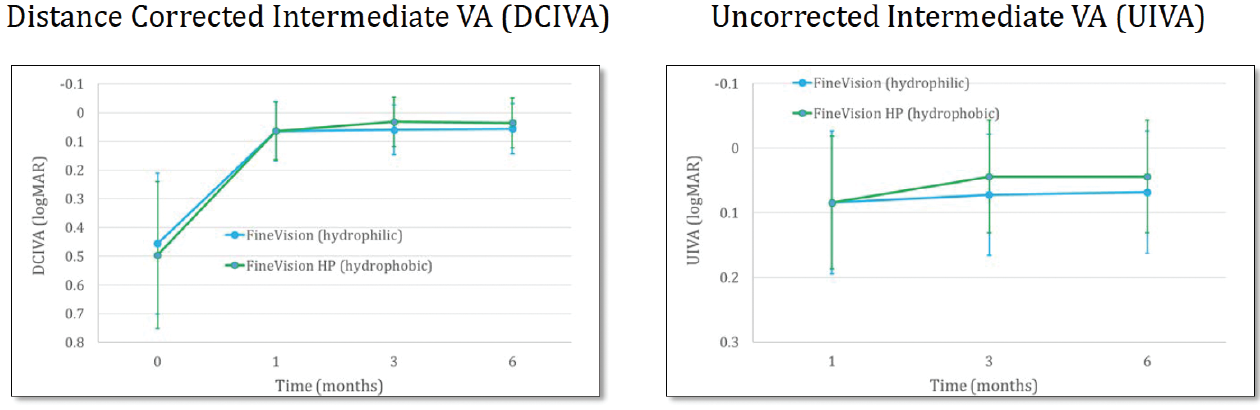
Figure 3. Intermediate visual acuity with the FineVision and FineVisionHP lenses.
To determine the defocus curve, we tested from a -3.50 to 0.90 D range. Both the hydrophilic and hydrophobic FineVision lenses achieved nice defocus curves for near, intermediate, and distance vision, and again both figures run parallel to each other so there was no statistically difference between the two types of lenses (Figure 4).
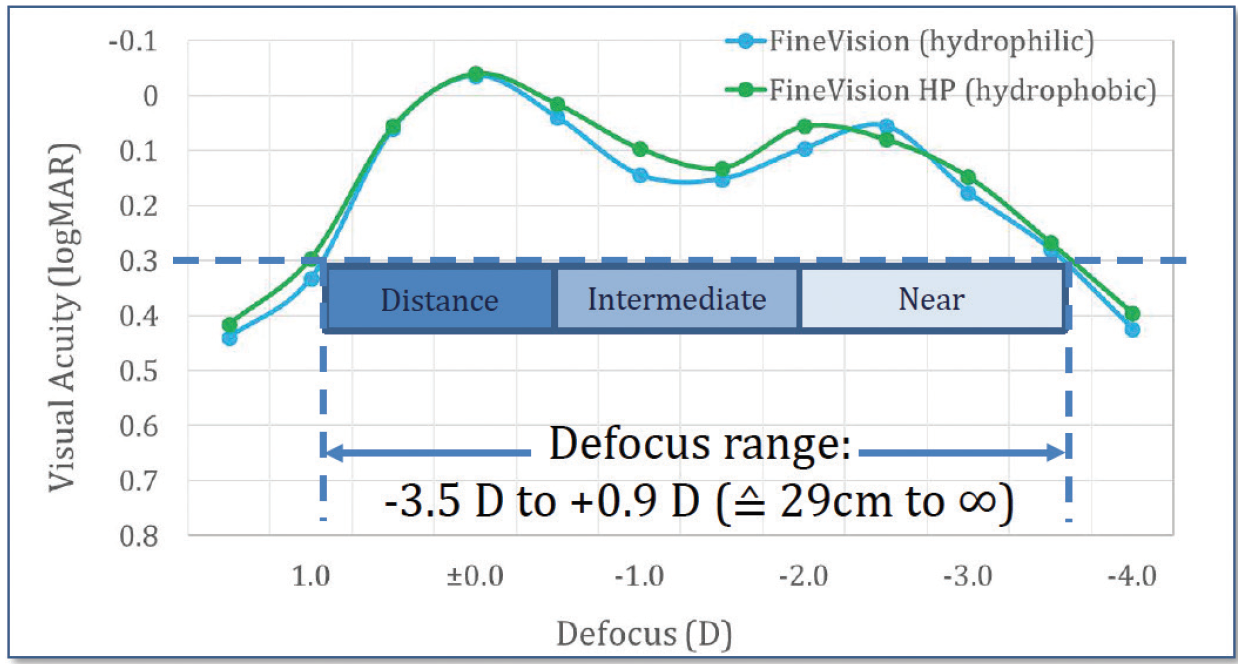
Figure 4. Near, intermediate, and distance vision defocus curves with the FineVision and FineVisionHP lenses.
We also looked at contrast sensitivity, which is a very important topic when one is discussing multifocal IOLs. At 3 months postoperative, contrast sensitivity was impressive. Because all patients were about 60 years old, the normal range is below what it would be in a phakic eye. In Figure 5, the normal range for a 60-year-old eye is shaded in gray color. In our study, all patients were above this range. Also, in mesopic conditions, all patients were within the normal range compared to nonoperated eyes. Visual acuity results with both IOLs were parallel as well, and there was no statistical difference between the hydrophobic and the hydrophilic material.
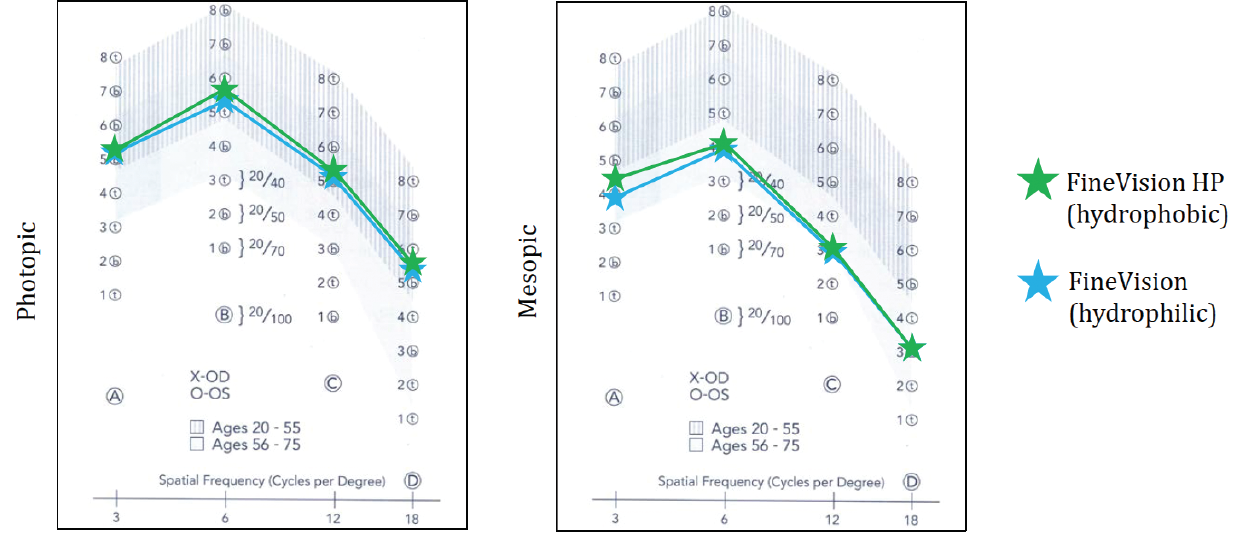
Figure 5. Contrast sensitivity in photopic and mesopic conditions with the FineVision (green) and FineVisionHP (blue) lenses.
At 6 months postoperative, UDVA was 0.11 ±0.13 and 0.10 ±0.10 with the hydrophilic and hydrophobic models, respectively. Further, DCIVA in these two groups was 0.16 ±0.08 and 0.14 ±0.08, respectively, and DCNVA 0.20 ±0.10 and 0.17 ±0.09, respectively.
CONCLUSION
The first clinical outcomes with the hydrophilic FineVision trifocal and the hydrophobic FineVisionHP were promising. Both lenses provided very good restoration of continuous visual acuity from near to far, and both showed good contrast sensitivity outcomes close to physiological values.
The new trifocal FineVisionHP is capable of providing the same unbeaten clinical outcomes proven by the FineVision hydrophilic lens, with the added benefits of a hydrophobic, glistening-free optic material. This material has been clinically tested for more than 7 years, showing very low rate of posterior capsular opacification and no glistenings.
