


Sponsored By

The use of the femtosecond laser for several important steps in cataract surgery is growing all over the world. Besides the known advantages, like the decrease in effective phaco time and the ability to correct corneal astigmatism with arcuate incisions done in the same procedure, the perfectness of the capsulotomy is another key advantage of the technology. There is significant clinical evidence that the laser capsulotomy is superior to the manual continuous curvilinear capsulorrhexis (CCC) regarding not only the roundness and centration but also in the postoperative result of the overlapping of the optic and the tilt of the lens. There seems to be also a potential benefit regarding the decrease in postoperative aberrations after laser-assisted cataract surgery (LACS) compared to routine surgery with phacoemulsification.
In our more than 3 years’ experience with LACS, the strength of the capsulotomy (Figure 1) and the incidence of capsular tears has been comparable to our results with CCC (personal data). Therefore, we have come to rely regularly on the use of the femtosecond laser for capsulotomy creation as well as other important steps in cataract surgery.
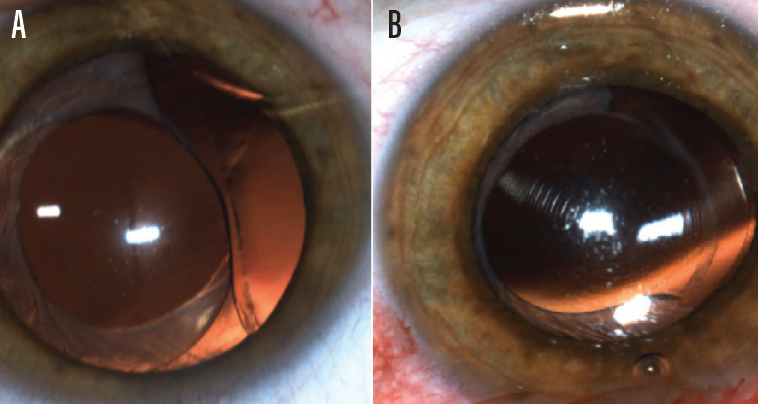
Figure 1. Decentration of a multifocal IOL, before (A) and after (B) rotation.
OPTIMIZING LENS FUNCTION
Surgical revision after cataract surgery due to problems with the IOL is fairly uncommon, but by far the largest reason for postoperative adjustments is lens decentration or tilt. This can occur because the capsulotomy size was either too big or too small or because phimosis of the capsulotomy occurred. With lens stability in the capsular bag playing an increasingly integral part in achieving excellent postoperative results, especially with premium IOL technologies, a perfectly round and appropriately sized capsulotomy with perfect centration becomes even more significant.
In addition to using the femtosecond laser to perform a capsulotomy with these characteristics, the femtosecond laser can also help to optimize IOL function in other ways. One example is when the laser capsulotomy is paired with an IOL designed to clamp into the capsulotomy, such as the FEMTIS IOL (Oculentis; Figure 2). In addition to two standard plate haptics, the FEMTIS lens design is characterized by four additional haptics that are enclaved in front of the capsulotomy. This eliminates the risk for the lens to dislocate postoperatively by becoming decentered or tilted.
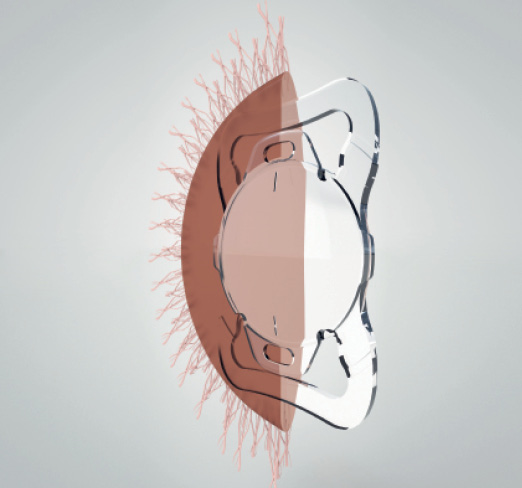
Figure 2. The design of the FEMTIS IOL.
LONG-TERM FOLLOW-UP
We now have 24-month follow-up in more than 90 eyes that have been implanted with the FEMTIS IOL. In all cases, the Lensar Laser System was used for capsulotomy and the CataRhex 3 system (Oertli) for phacoemulsification. A total of 66 patients were enrolled; the mean age in these patients was 75 years.
In all cases, there were no complications during lens implantation, and there were no cases of the lens becoming decentered postoperatively. Furthermore, the enclavation of the capsulotomy behind the additional haptics led to no complications, and the optic was free of any overlap with the anterior capsule in all cases.
Mean DCVA in the operated eye increased from 0.5 decimal preoperatively to 0.91 ±0.22 decimal postoperatively; mean binocular DCVA was 1.0 ±0.26 decimal.
We also looked at pigment dispersion, as the four additional haptics are placed in front of the capsular bag, touching the pigment. There was no evidence of this postoperatively, and, at 24 months, no eyes had experienced problems with pigment epithelium or pigment glaucoma (Figure 3). Further, IOP had decreased to 13.79 ± 3.0 mm Hg by 24 months postoperatively, from 16.6 ±1.73 mm Hg preoperatively.
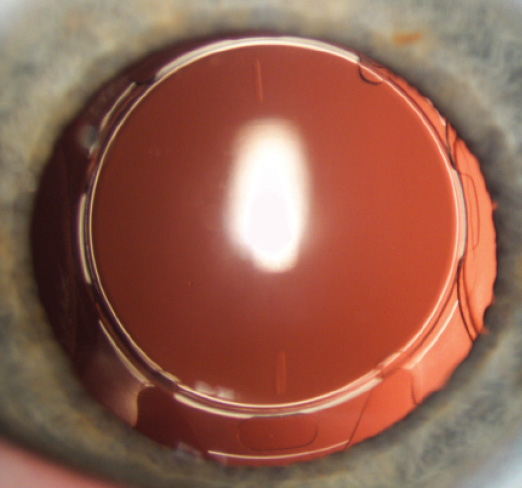
Figure 3. FEMTIS IOL in situ, 24 month after implantation.
We have found the design of the FEMTIS IOL to be very stable, with no signs of postoperative rotation; this will be of great benefit in any future toric and multifocal IOL designs. Additionally, the fact that the lens optic does not overlap with the anterior capsule, leading to fewer symptoms of dysphotopsia, may be advantageous in younger patients and in those with large pupils. We have started to use the Comfort EDOF version of the FEMTIS IOL with 1.50 D addition recently. Our results in this series have been promising, but longer-term follow-up and a prospective comparison to the standard model must be conducted.
BEST PRACTICES
Below I offer four best practices with the FEMTIS IOL.
Best practice No. 1: Capsulotomy size. The total diameter of the aspheric FEMTIS lens, made of hydrophilic acrylic material, is 10.5 mm, and the optic diameter is 5.7 mm. In my experience, it should be clamped into a Lensar laser capsulotomy of about 4.8 to 5 mm in order to achieve the best results. After consultation with colleagues using other femtosecond laser systems, it seems that we have a difference between adjusted capsulotomy sizes for a perfect enclavation behavior of the FEMTIS IOL. For example, the LenSx (Alcon) needs to be an entered capsulotomy size of about 5 to 5.2 mm to easily fixate the additional haptics of the lens.
Best practice No. 2: Positioning the additional haptics. Thus far in my experience with the FEMTIS, totaling about 100 implantations, I have not had one lens-related complication. The only learning curve I experienced was figuring out how to position the four additional anterior haptics (two large longitudinal and two smaller latitudinal) into the capsulotomy to secure and center the IOL, but it was very short. Through my experience I have found that, by adding a simple Sinskey hook to the other instruments I use during lens implantation, I am able to position the FEMTIS IOL quite well.
Best practice No. 3: Implant the IOL under an OVD. After insertion of the lens into the capsular bag, it is important to aspirate the OVD completely from behind the lens. Subsequently, using an OVD when enclaving the additional four haptics is useful. Of particular note is the importance of removing the OVD completely after the haptics are in position.
Best practice No. 4: Use Mydriasert. I have found it helpful to use Mydriasert (tropicamide and phenylephrine HCl; Thea Pharmaceuticals) to expand the pupil every time I perform LACS. Enlarging the pupil size to greater than 6 mm facilitates ease of enclavation and reduces the risk for iris capture.
CONCLUSION
We believe that every patient who elects LACS is a candidate for the FEMTIS IOL. More specifically, those with high myopia and large-diameter capsular bags often do well with this design, as there is less risk of IOL decentration postoperatively. I do not recommend this lens to be used with a Lensar laser capsulotomy of less than 4.5 mm, as enclavation of the haptics becomes too tricky. Also, because the IOL has plate haptics, it is not recommended to implant the FEMTIS IOL in patients with loose zonulas.
With those two caveats, I believe that, compared with standard IOL designs, the FEMTIS lens has many advantages. The biggest advantage is that it allows perfect centration of the lens to the center of capsulotomy.
