
A circular opening in the lens capsule is a gateway inside the eye for cataract surgery. For years, the most common technique to open the capsule was a manual capsulorrhexis, with handheld forceps introduced through the main or sideport incision to punch the capsule and create the circular opening. As we have come to learn, the size and shape of the capsular opening can play an integral role in postoperative outcomes and in IOL centration. Although the manual capsulorrhexis is extremely effective, it is not always circular and, occasionally, can be smaller or larger than the IOL optic, thereby compromising long-term IOL stability.
More recent innovations, such as the femtosecond laser, can be used to cut the capsule with higher precision than a manual technique, producing a so-called free-floating capsulotomy. The femtosecond laser is especially advantageous today, as more premium lens technologies, which rely on a precise capsulotomy for long-term IOL centration, are being implanted. There are drawbacks to the use of current femtosecond laser platforms for cataract surgery, however. These include that the systems are bulky, they are expensive, and they also can require a dedicated operating room. Such burdens have contributed to the prevention of widespread use of femtosecond laser technology.
Nevertheless, due to the highly predictable size, shape, and position of the laser capsulotomy, the femtosecond laser has been found to be a helpful tool to improve IOL centration. In fact, it can be combined with a lens designed for use with a laser capsulotomy, the FEMTIS IOL (Oculentis), to achieve even better centration and, thus, better postoperative outcomes. The FEMTIS IOL is currently in clinical trials, in which I am participating.
A compact, cheaper alternative to the femtosecond laser for capsulotomy creation is the CapsuLaser (CapsuLaser). This device, mounted under the surgical microscope, can create a precise and reliable capsulotomy with a firm and elastic edge in about 1 second. Laboratory measurement has shown that the CapsuLaser capsulotomy is significantly more stretchable than a manual capsulorrhexis.1 I recently began using the CapsuLaser device with the FEMTIS IOL, and to date my results have been impressive. Thus far, I have implanted about 30 monofocal and 10 multifocal lenses in combination with the CapsuLaser.
SURGERY
After trypan blue dye is washed out of the eye, the anterior chamber is filled with OVD. Then, the aiming beam is focused through the handheld contact lens of the CapsuLaser, and the laser is focused by a footswitch. The capsulotomy is then performed in 1 second.
The central capsule is removed, followed by cataract removal. The FEMTIS IOL, which is designed for optic fixation in the laser capsulotomy by means of dedicated microhaptics, is placed in the cartridge and implanted through a 1.8- to 2-mm incision (Figure 1), depending on the power of the lens to be implanted. Before fixating the FEMTIS optic into the capsulotomy, the leading haptics are introduced straight into the capsular bag and the trailing haptic into the anterior chamber. Then, the trailing haptic is manipulated to the capsular bag. The next step is to clip the large haptic onto the capsule at the 6-o’clock position, followed by the microhaptic at the 12-o’clock position (Figure 2). Finally, the smaller haptics are manipulated in front of the capsule at the 3- and 9-o’clock positions (Figure 3). The IOL optic is perfectly fixed in the capsule opening, promoting reliable IOL centration and preventing IOL rotation (Figure 4).
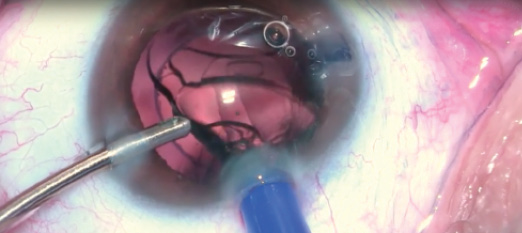
Figure 1. The FEMTIS IOL is inserted into the capsular bag.
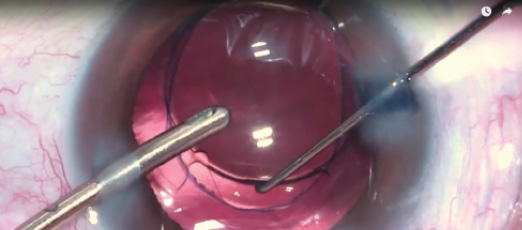
Figure 2. One of the large haptics is clipped onto the capsule.
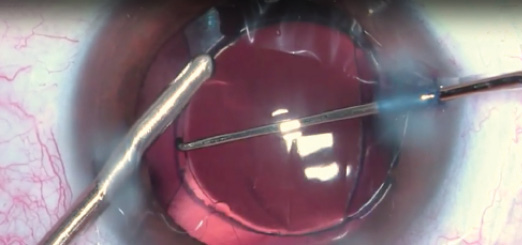
Figure 3. The smaller haptics are manipulated in front of the capsule.
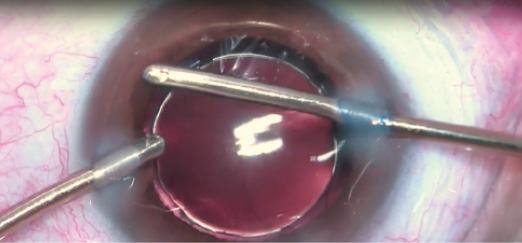
Figure 4. The IOL is perfectly fixed in the capsule opening.
ADVANTAGES AND TIPS
I first used the FEMTIS IOL combined with the CapsuLaser 2 years ago. In this time, I have noticed advantages and learned valuable tips.
Advantage No. 1: The CapsuLaser creates a perfect and well-centered capsulotomy, and the IOL is always well-centered. In my experience, there is virtually no movement or rotation of the IOL after the haptics are in place and the microhaptics are clipped onto the capsulotomy.
Advantage No. 2: An alternative to implanting the FEMTIS IOL under OVD is that it can be implanted with a hydro-assisted implantation technique. The advantage to this technique is that there is no OVD to aspirate from both the capsular bag and the anterior chamber after the lens is implanted. This makes surgery shorter.
Advantage No. 3: The design of the IOL eliminates almost all presence of dysphotopsias. This includes rainbows, streaks, crescents, rings, halos, glare, haze, and fog.
Tip No. 1: The FEMTIS IOL will work better with slightly larger capsulotomy performed with the CapsuLaser. In my hands, I size the capsulotomy between 5 and 5.2 mm.
Tip No. 2: Use trypan blue dye. Staining improves visibility of the capsular edge for the entire surgery, including IOL fixation.
Tip No. 3: Center on the visual axis. When using the CapsuLaser to create the capsulotomy, the FEMTIS should be centered on the visual axis, not the pupil.
Tip No. 4: Personalize your A-constant. At first, I used the A-constant that was suggested by Oculentis. Over time, I figured out that adding 0.1 to the A-constant produced even better results.
I implanted the FEMTIS IOL in a professional truck driver who often drives at night. Surgery was uneventful (http://bit.ly/stodulka1017), and, by 1 month postoperative, he had achieved 20/20 binocular UCVA, with -0.75 D cylinder in his left eye. By 3 months, the patient reported that he had no problems with glare or halos and no negative dysphotopsias. Upon clinical evaluation, I noted that the circular capsulotomy continued to hold the IOL in place (Figure 1). The microclips, which remained well positioned on the capsulotomy edge, had very little fibrosis (Figure 2), and there were no signs of secondary capsular opacity (Figure 3) or posterior capsular opacification.
Figure 1. The IOL is held in place by the circular capsulotomy.
Figure 2. The microclips are well positioned on the capsular edge.

Figure 3. No signs of secondary capsular opacity.
CONCLUSION
Laser capsulotomy serves as a perfect support for premium IOLs and creates a platform for excellent long-term IOL centration. In my experience, fixating the FEMTIS IOL on the capsulotomy opening of the anterior capsule is straightforward, with little additional surgical time.
The combination of a CapsuLaser capsulotomy and the FEMTIS IOL is a promising new way to provide patients with excellent postoperative outcomes, to create a stable lens position, and to promote long-term IOL centration.
1. Packard R. A new approach to laser capsulotomy. CRST Europe. https://crstodayeurope.com/articles/2015-oct/a-new-approach-to-laser-capsulotomy. Accesed July 4, 2017.
