
I started using the FEMTIS IOL (Oculentis) in 2014, when it first became available, as part of a multicenter clinical trial. At the time, I was practicing at the University of Heidelberg, one of nine centers participating in the multicenter trial. Like my colleagues, I was impressed with the results we had with the IOL, and it was an easy technology to incorporate into practice. About 2 years ago, however, I started working at a new practice, Eyeclininc Ahaus-Raesfeld-Rheine, and I no longer had access to a femtosecond laser. As a result, I had to set aside the FEMTIS IOL, simply because it was not beneficial to implant without a femtosecond laser capsulotomy to clip it into—or so I thought.
About 2 months ago, Eyeclininc Ahaus-Raesfeld-Rheine purchased the Zepto Precision Pulse Capsulotomy device (Mynosys). From the first time that I used it, I found the capsulotomy produced by the Zepto was far more stable than a manual capsulorrhexis. I also noticed that the capsulotomy was much easier to stretch than the capsulotomy created manually or by a femtosecond laser.
The lightbulb immediately went off: Would it be possible to implant the FEMTIS IOL into a capsulotomy created by the Zepto? The FEMTIS lens has two standard plate haptics and four additional haptic flaps, or microhaptics, on the periphery on the lens optic. The two plate haptics are positioned in the capsular bag, and the four microhaptics pull over the edge of the capsulotomy, so that the whole lens is enclaved in the capsulotomy. Because of the stretchiness of the Zepto capsulotomy, I thought it would be an ideal combination with the FEMTIS IOL.
I spoke to Oculentis about my idea and asked if I could be the first to try implanting the FEMTIS within the Zepto-created capsulotomy (Figure 1). I was keen to do this because, the more I used the Zepto, the more I was convinced that the capsulotomy was far superior to those created manually or even with the femtosecond laser. Once I got the okay from Oculentis, immediately I lined up my first case.
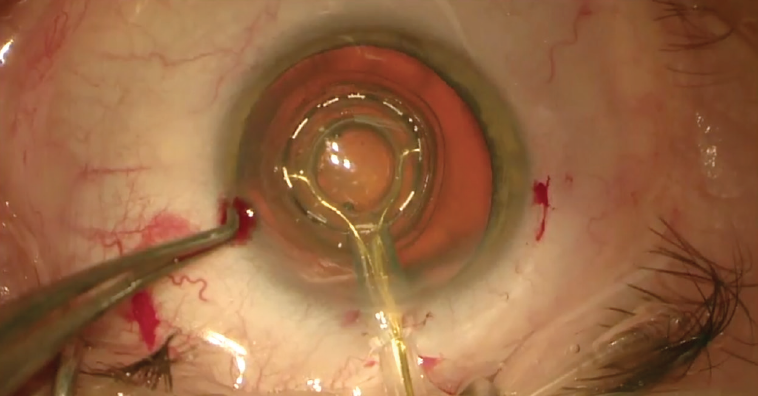
Figure 1. The Zepto is used to create a capsulotomy.
CURRENT EXPERIENCE
I am the only person using the combination of the FEMTIS IOL and the Zepto, and to date I have completed four cases. Even with little clinical experience, I have already noticed several benefits. First, with regard to the FEMTIS IOL, I do not need to implant the lens under an OVD. Many surgeons do use an OVD during lens implantation, but with this lens I can use balanced saline solution, which unlike OVD does not have to be removed from the anterior capsule and from behind the IOL. One of the largest advantages this affords is that there is no chance of IOL rotation or decentration during aspiration (Figure 2).
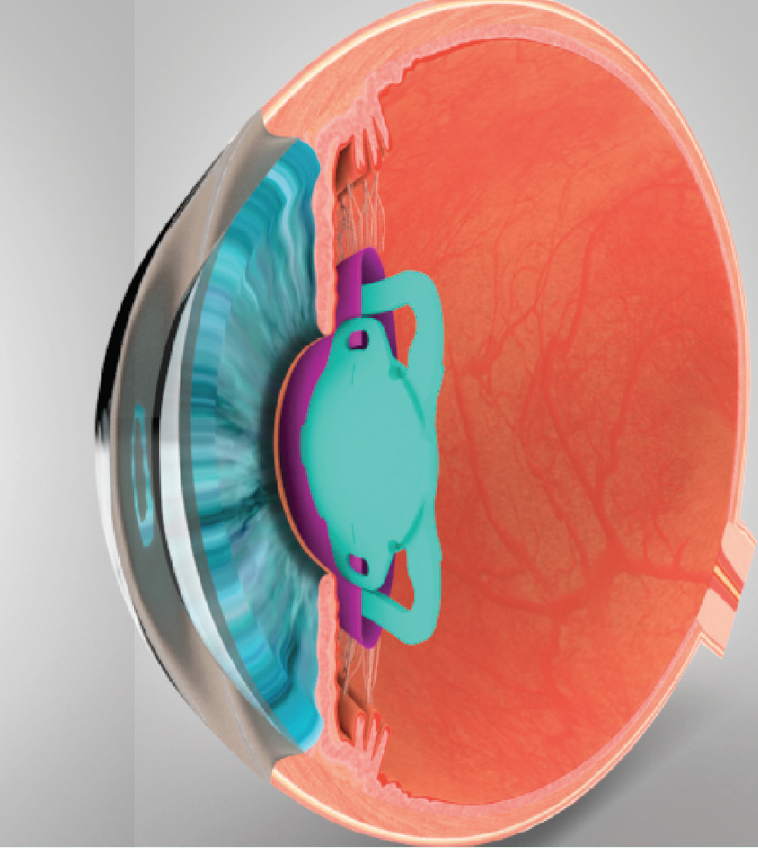
Figure 2. Due to the positioning of the FEMTIS IOL in the capsulotomy, there is no chance of IOL rotation or decentration.
Second, with regard to the Zepto, it is also possible to implant the FEMTIS IOL in eyes with small pupils. In these cases, the Zepto is simply placed underneath the iris. Third, the Zepto creates the capsulotomy in one complete motion, whereas with the femtosecond laser it is created with several. As a result, the femtosecond capsulotomy can have perforations that enlarge to tags.
PEARLS WITH THE ZEPTO AND FEMTIS
Centration. Centration of the Zepto capsulotomy can be a little bit challenging. There is a wire inside the device to guide the treatment; that wire is pulled back to apply the vacuum. If pulled too quickly, the suction cap of the device could shift, and the capsulotomy could become decentered. I recommend pulling the wire back with the vacuum pump already switched on. This will ensure that there is immediate suction on the anterior capsule when the wire is gone and that the device stays in place. Otherwise, the concept of the FEMTIS IOL—being locked in the capsulotomy in a stable position—is not advantageous, as it might be dencentered. Using this trick ensures the lens is positioned on the optical axis, whereas an intracapsular IOL would center on the capsular bag.
Patient selection. Another pearl is regarding patient selection. The FEMTIS IOL can be implanted in any eye in which a monofocal IOL is appropriate; however, I do recommend that the anterior chamber depth be around 2 mm if using the Zepto, so that there is enough space for the Zeptodevice to go inside and also for the instruments to fixated the FEMTIS IOL in the anterior capsulotomy.
CONCLUSION
In the little more than 2 months that I have been using the Zepto Precision Pulse Capsulotomy device, I have come to the conclusion that the capsulotomy it creates is more stable than the manual capsulorrhexis or the femtosecond capsulotomy and, therefore, more prudent for use with the FEMTIS IOL.
