
It is no secret that today’s cataract surgery patients have high expectations for their postoperative vision, and it is not uncommon for them to come in desiring spectacle independence. Unfortunately, though, there is no single IOL that we can offer that provides the crisp, clean spectacle-free vision that patients enjoyed as 20-year-olds. Every IOL has trade-offs, so to speak, and I have experimented with many different models in attempt to find the perfect solution for my patients.
Most recently, my experimentation has led me to the FEMTIS IOL (Oculentis), which I have been using for the past year. When combined with laser-assisted cataract surgery (LACS), the three major benefits of the IOL are: (1) excellent centration and stability, (2) perfect overlap of the rhexis and the optic, and (3) excellent refractive outcomes. In essence, these benefits are all afforded by the IOL’s special haptics system, which allows the lens to be clamped into the capsulotomy.
The promise of an IOL that can achieve a consistent effective lens position and promote the absence of IOL tilt is attractive as the next step forward in IOL design. Currently, I consider the FEMTIS IOL in any patient in whom a monofocal IOL is indicated. In the future, as toric and multifocal IOL models of the FEMTIS become available, I will further extend the indications in which I recommend this platform. In my opinion, these future uses of the FEMTIS technology are even more exciting.
STUDY
I am currently investigating the FEMTIS IOL as part of a multicenter study to determine the lens’ safety and efficacy. Thus far, in total, 163 patients have been enrolled across nine centers. Specifically at Midland Eye, we have already enrolled 50 eyes. In all cases, the FEMTIS IOL was implanted bilaterally in patients between the ages of 67 and 88 (mean, 76.96 ±6.35 years) with a target refraction of plano. The Haigis formula was used to calculate IOL power, and the mean IOL power was 20.50 D.
Patients were examined preoperative and at 1 to 7 days, 6 to 8 weeks, 6 and 12 months postoperatively. The main endpoints of the study were IOL decentration, rotation, tilt, the distance between the iris and the IOL, refraction, and visual acuity.
Surgery was uncomplicated in all cases. After pupil dilation with Mydriasert (tropicamide and phenylephrine HCl; Thea Pharmaceuticals), the Lensar Laser System (Lensar) was used to create a capsulotomy with a diameter of 4.9 to 5 mm; it was also used for lens fragmentation. A manual corneal incision of about ≥2.4 mm was made to aid in lens implantation.
Once the FEMTIS IOL was positioned completely in the bag, OVD was aspirated from behind the IOL, through the small optic holes (Figure 1). The lens’ two large longitudinal haptics, followed by the two small lateral haptics, were then enclaved in the capsulotomy. Miochol-E (acetylcholine chloride intraocular solution; Bausch + Lomb) and pilocarpine 2% were instilled.
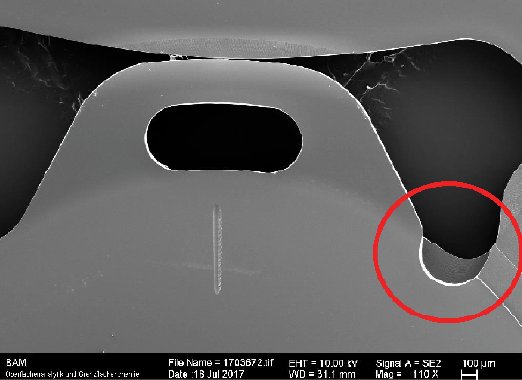
Figure 1. The small optic hole of the FEMTIS IOL.
There was virtually no learning curve with the FEMTIS IOL. Although it might take a little more time to implant due to the need to flip the haptic flaps of the IOL over the anterior capsule once the lens is in the bag, implantation is quite straightforward. The lens is injected through a standard injector system and behaves just like the rest of the Oculentis IOLs. When starting with this lens, however, I would recommend selecting patients with good pupil dilation.
RESULTS
All eyes were available for follow-up through 6 months. At 12 months, only 24 eyes were available. Generally speaking, the results are impressive because they are better than one would typically expect to achieve in this age group with a standard monofocal IOL. Furthermore, although patients did not have any means to compare their vision with this IOL and another—since the FEMTIS was implanted bilaterally—all were happier than one would normally expect patients in a monofocal IOL study to be.
Days 1 to 7. At the first follow-up, the mean UCVA was 0.14 ±0.19 logMAR, which is better than 20/32 on the Snellen chart. Although iris capture with the haptics occurred in eight eyes, all were early in our learning curve. Of these, four resolved with pupil dilation and four required repositioning of the IOL.
Weeks 6 to 8. By 6 to 8 weeks postoperatively (Figure 2), mean UCVA improved to 0.05 ±0.15 logMAR, which is better than 20/25 on the Snellen chart. Furthermore, the mean BCVA was -0.05 ±0.10 logMAR, which is better than 20/20 on the Snellen chart. The mean sphere, cylinder, and spherical equivalent (SE) were 0.53 ±0.51 D, -0.83 ±0.41 D, and 0.27 ±0.36 D, respectively. There was one case of mild cystoid macular edema and one inferior curvature to the optic edge.
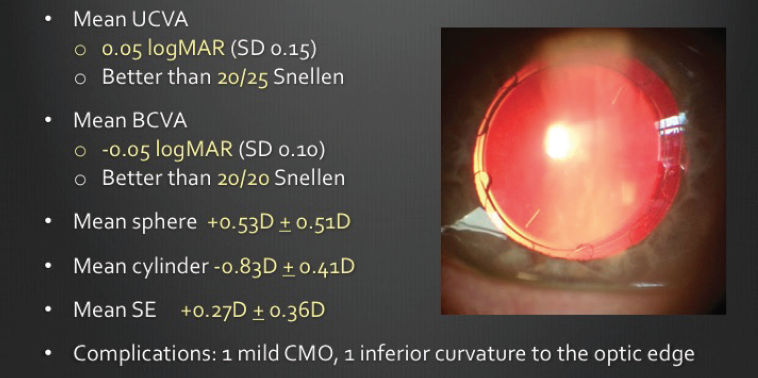
Figure 2. Six to 8 weeks postoperative visit.
Month 6. At 6 months postoperatively (Figure 3), the mean UCVA remained stable and was still better than 20/25 on the Snellen chart (0.08 ± 0.14 logMAR). The mean BCVA had improved slightly to -0.04 ±0.08 logMAR, which is about 20/16 on the Snellen chart. The mean sphere, cylinder, and SE at this follow-up were 0.70 ±0.51 D, -0.68 ±0.48 D, and 0.43 ±0.42 D, respectively.
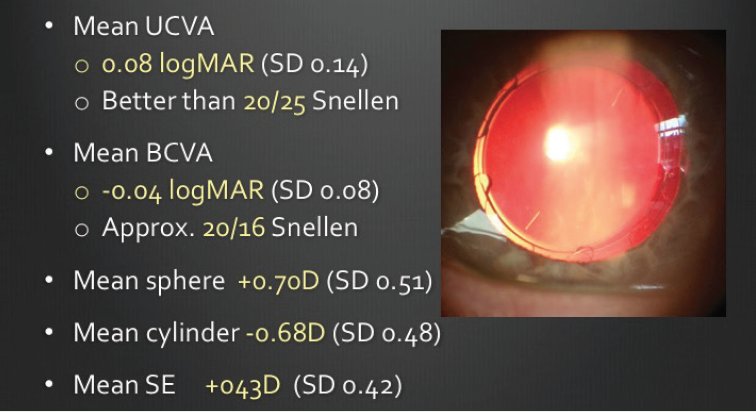
Figure 3. Six month postoperative visit.
Month 12. In addition to mean UCVA (0.05 ±0.16 logMAR; better than 20/25 Snellen), BCVA (-0.05 ±0.1 logMAR; better than 20/20 Snellen), sphere (0.60 ±0.38 D), cylinder (-0.66 ±0.26 D), and SE (0.40 ±0.30 D), we also looked at the incidence of posterior capsular opacification (PCO) at 12 months postoperative (Figure 4). A score of zero indicated no PCO, whereas a score of 4 indicated PCO spread across the entire visual axis; the mean score was 0.39 ±0.48.
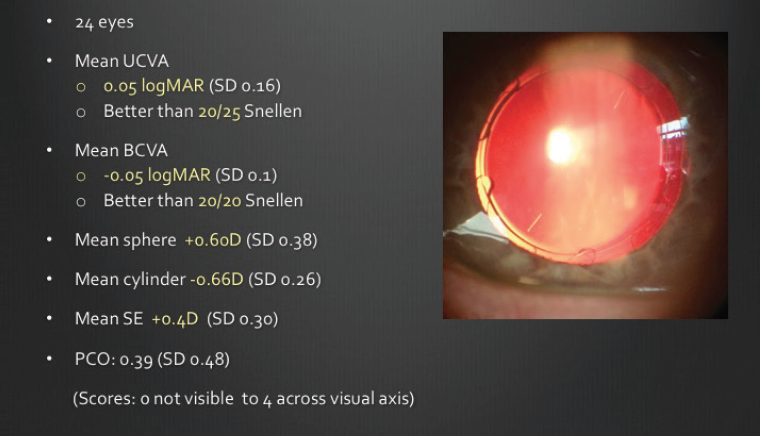
Figure 4. Twelve month postoperative visit.
CONCLUSION
As our study results have shown thus far, the FEMTIS IOL is not only capable of achieving excellent refractive outcomes but of also achieving exceptional centration and stability (Figure 5) and perfect overlap of the rhexis and the optic. Although we only have a small subset of patients who have completed 12-month follow-up, our results in the current FEMTIS IOL study are significantly better than the results of other clinical trials with 12 months’ follow-up, including the UK National Cataract Survey, the National Eyecare Outcomes Network, the Swedish National Cataract Register, and the Cataract National Dataset Electronic Multicentre Audit.
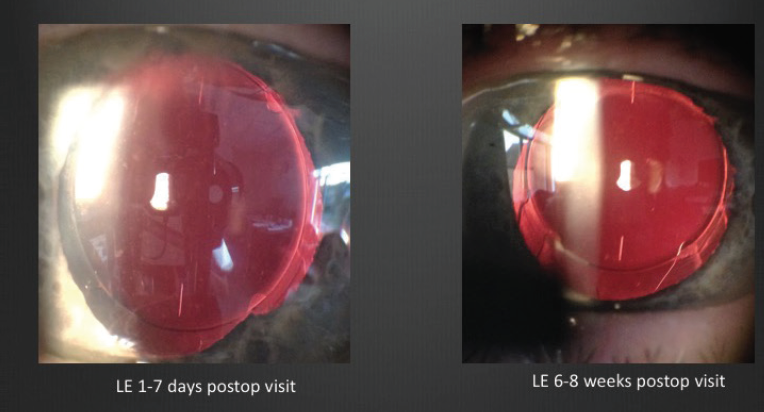
Figure 5. At all time points, the FEMTIS IOL was centered and stable.
Even more exciting than our current outcomes is the promise that the FEMTIS IOL platform holds for the future, once toric and multifocal versions emerge.
