
A 37-year-old man presented to the London Vision Clinic in May 2013 for a corneal laser refractive surgery consultation. He had a history of congenital nystagmus, and previous attempts to wear both soft and gas permeable contact lenses were unsuccessful. On examination, his manifest refraction was -0.50 -6.00 X 137º (20/40-1) OD and -2.25 -2.25 X 30º (20/40-1) OS. Preoperative corneal topography (ATLAS 9000, Carl Zeiss Meditec) and tomography (Orbscan IIz, Bausch + Lomb; Pentacam, Oculus Optikgeräte) were normal. The patient’s contrast sensitivity (CSV-1000, VectorVision) was below normal at 3 cycles/degree (cpd) and recorded as none at 6, 12, and 18 cpd in both eyes. Central corneal thickness with handheld ultrasound pachymetry (Corneo-Gauge Plus, Sonogage) was 537 µm OD and 533 μm OS. A slit-lamp examination and dilated fundus examination were unremarkable. The patient was found to be a suitable candidate for corneal laser refractive surgery. Given his nystagmus and the possibility for dynamic tracking errors during LASIK, it was decided that small-incision lenticule extraction, or SMILE, was the safest option. The entire refractive portion of the treatment is performed with the eye immobilized under suction, which would be particularly advantageous in this case.
Surgery
SMILE was performed using the 500-kHz VisuMax femtosecond laser (Carl Zeiss Meditec). In SMILE, the alignment of the refractive lenticule is effectively autocentered while the patient fixates coaxially on a fixation light prior to suction being applied. This results in the lenticule formation centered on the corneal vertex of the coaxially fixating eye.1 During the docking process, it is important to verify that centration is achieved on the visual axis, which can be achieved using the position of the reflex from the green fixation light as a reference in relation to the pupil. To help this process, we prepare a printout for every patient, which includes the topographical image of the eye and the Hirschberg test (Figure 1). (Note: A template is available to download from www.londonvisionclinic.com/SMILECentrationTemplate). The surgeon can then compare this to the intraoperative appearance. If the achieved centration does not appear to match the prepared rings image, the contact glass can be released and docking can be attempted again.
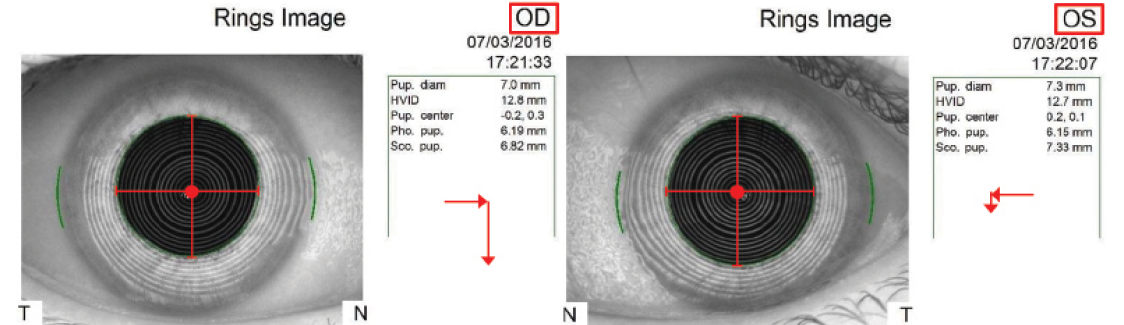
Figure 1. Example of the printout used as a reference to the expected position of the corneal reflex during docking. The corneal vertex (center of the Mires rings) is indicated as a red dot, with red cross-hair guidelines overlaid to visualize the position relative to the pupil border. A further visual cue is included in the form of arrows, which represent the magnitude and direction of the corneal vertex relative to the center of the entrance pupil, as defined by the coordinates measured by the Atlas. (Figure reprinted with permission from Reinstein DZ, Archer TJ, Carp GI. The Surgeon’s Guide to Small Incision Lenticule Extraction (SMILE). Thorofare, New Jersey: SLACK Incorporated, 2018.)
Particular care and attention was required during docking for this patient due to the involuntary nystagmus eye movements. Fortunately, as the eye comes into contact with the contact glass, this pressure limits the movements and the routine centration fine-tuning can take place, cross-checking against the topographical image guide as described above. Proper centration was achieved on the first attempt in this eye, but docking could have been repeated multiple times if necessary. The cornea was then immobilized for the entirety of the lenticule creation, thus achieving perfect treatment centration.
A SMILE procedure for an eye with nystagmus with high refractive cylinder of -6.00 D.
Reproduced with permission from Reinstein DZ, Archer TJ, Carp GI. The Surgeon’s Guide to Small Incision Lenticule Extraction (SMILE). Thorofare, New Jersey: SLACK Incorporated, 2018.
The lenticule interface separation and extraction was performed using our standard technique.2 In this case, the optical zone diameter was 6.75 mm, cap thickness was 130 μm, and cap diameter was 7.95 mm in both eyes. A primary 2-mm superotemporal small incision and a reserve superonasal 2-mm small incision were created in both eyes.
Outcome
One year after surgery, the patient reported no subjective complaints and had a distance UCVA of 20/40 OD with a manifest refraction of +0.25 -0.25 X 130º and 20/40 OS with a manifest refraction of +0.25 DS. An OCT B Scan (RTVue, Optovue) was normal, and there was no tissue irregularities at the interface level in either eye (Figure 2). Corneal topography was also regular in both eyes, and the difference map for the patient’s right eye (high cylinder treatment) showed a perfectly centered treatment (Figure 2). The contrast sensitivity was unchanged from before surgery.
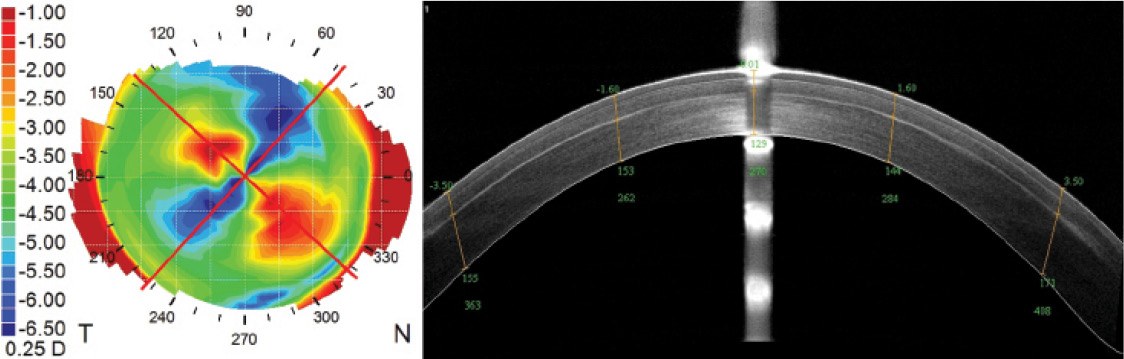
Figure 2. Atlas topography difference map (left) and OCT B scan at 1-year postoperative (right) of the patient’s right eye. The Atlas is overlaid with red lines that indicate the axis of the intended cylinder correction, which are perfectly aligned with the achieved corneal astigmatic change. The irregularities in the difference map are due to the nystagmus during topography acquisition. The B-scan shows a regular and smooth interface.
Conclusion
In this example, a patient with both nystagmus and high astigmatism was successfully treated with SMILE by taking advantage of the eye being immobilized by the suction during lenticule creation. SMILE in eyes with nystagmus is a feasible treatment option and may provide even better centration control compared to standard eye-tracking software used in LASIK and PRK.
In eyes with high astigmatism such as in this case, a more recent advance is to use corneal marks to control for cyclotorsion.3,4 Once suction has been applied and centration has been deemed satisfactory, the surgeon can compare the location of the marks on the horizontal and vertical corneal diameter to the cross-hairs of the reticle on the planning screen. If any rotation is required, the surgeon can simply hold the contact glass and rotate it until the marks are aligned; the cornea will be rotated in turn due to the suction.
1. Reinstein DZ, Gobbe M, Gobbe L, Archer TJ, Carp GI. Optical zone centration accuracy using corneal fixation-based SMILE compared to eye tracker-based femtosecond laser-assisted LASIK for myopia. J Refract Surg. 2015;31:586-592.
2. Reinstein DZ, Archer TJ, Carp GI. The Surgeon’s Guide to Small Incision Lenticule Extraction (SMILE). Thorofare, New Jersey: SLACK Incorporated, 2018.
3. Jun I, Kang DSY, Reinstein DZ, Arba-Mosquera S, Archer TJ, Seo KY, Kim TI. Clinical outcomes of SMILE with a triple centration technique and corneal wavefront-guided transepithelial PRK in high astigmatism. J Refract Surg. 2018;34:156-163.
4. Ganesh S, Brar S, Pawar A. Results of intraoperative manual cyclotorsion compensation for myopic astigmatism in patients undergoing small incision lenticule extraction (SMILE). J Refract Surg. 2017;33:506-512.



