

A 40-year-old woman with congenital aniridia was referred to me for a cataract surgery consultation. On presentation, she had bilateral polar posterior cataracts, amblyopia, foveal hypolplasia, borderline ocular hypertension, and astigmatism. The patient was also experiencing symptoms of dry eye disease, another common comorbidity in patients with aniridia. Preoperative imaging with the Eyestar 900 (Haag-Streit) is shown in Figure 1.
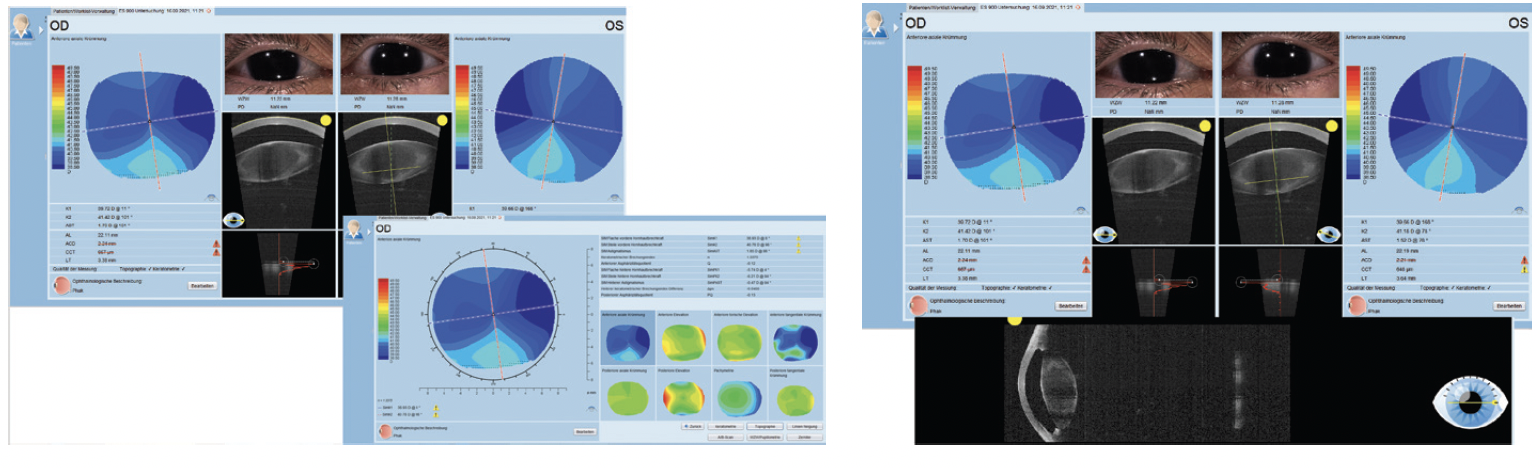
Figure 1. Preoperative imaging in the right and left eyes with the Eyestar 900.
The biometry measurements, also taken with the Eyestar 900, both showed that both eyes had a short axial length (22.11 mm OD and 22.19 mm OS) and a very shallow anterior chamber (ACD; 2.21 mm OD and 2.24 mm OS; Figure 2). Both corneas were also flat.
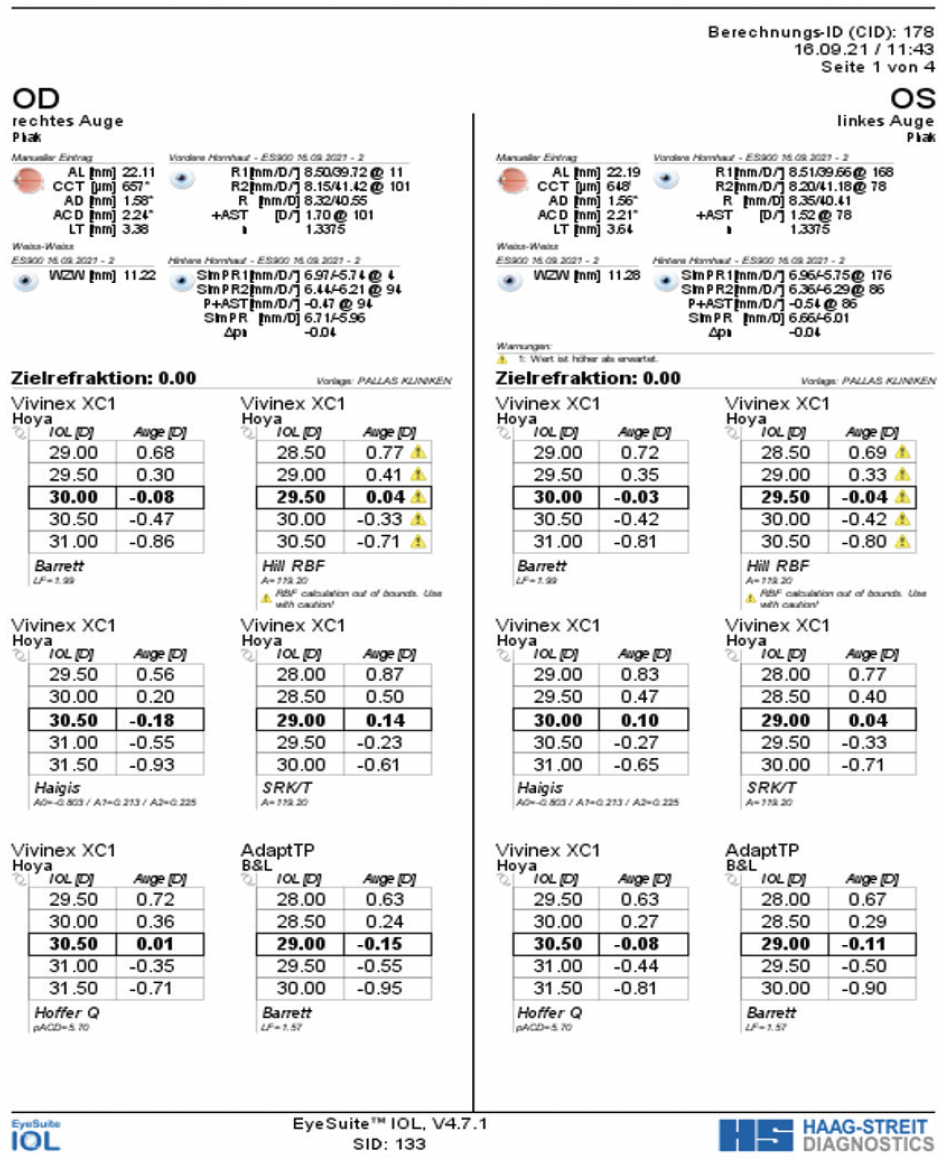
Figure 2. Biometry measurements with EyeSuite Software.
This article details the possible use of the Eyestar 900 powered by EyeSuite analysis software to measure the lens diameter. It also demonstrates how collaboration with Haag-Streit helped to produce a successful outcome in a challenging case.
SURGICAL PLANNING
The patient was scheduled for bilateral cataract surgery and implantation of a CustomFlex ArtificialIris Fiberfree (HumanOptics) and capsular tension ring—a standard practice for me in eyes with congenital aniridia—in her left eye first.
IOL power. The IOL chosen was a Vivinex XC1 (Hoya Surgical). In this case, the IOL power calculations for the closest target refraction to emmetropia with the Eyestar 900 for the left eye varied from 29.00 D with the SRK/T to 30.50 D with the Hoffer Q. The Hill-RBF and Barrett and Haigis formulas showed IOL powers of 29.50 and 30.00 D, respectively. I selected a lens power of +29.50 D for the left eye that resulted in a spherical equivalent (SE) of -0.375 D and calculations according to Hill-RBF was a SE of -0.04 D.
In the right eye, again the IOL power calculations varied from 29.00 D to 30.50 D. For this eye, the SRK/T calculation produced an IOL power of 29.00 D, the Hill-RBF an IOL power of 29.50 D, the Barrett an IOL power of 30.00 D, and the Haigis and Hoffer Q an IOL power of 30.50 D. I selected an IOL power of +30.00 D that resulted in a SE of +0.25 D and calculations according to Barrett was a SE of -0.08 D.
Artificial iris implantation. I usually prefer the ArtificialIris to be implanted in the sulcus. For eyes with congenital aniridia, however, I like to implant it in the capsular bag to avoid touching the ciliary structures and decrease the risk for inflammation and glaucoma. Implantation in the capsular bag requires some extra work because the implant should fit perfectly in the capsular bag. If too small, the pupil will be decentered inferiorly; if the chosen size is too large, the implant might become folded and damage the capsule.
To determine the perfect size of the implant, I worked with Haag-Streit to manually measure the diameter of the lens capsule. In the case of a complete aniridia, no obstruction on the OCT imaging is present. Hence, the lens can be imaged from equator to equator. By using the Eyestar’s OCT scans of the patient’s eye, I outlined the lens capsule (Figure 3) in all radial scans and sent the images to the company to determine the diameter. Haag-Streit then calculated from these radial scans the average diameter to be 9.84 mm in the right lens and 9.64 mm in the left. I trephined the ArtificialIris to 9.5 mm for implantation in the capsular bag. An interesting fact to note: The average normal lens weighs 220 mg (including the capsular bag). The IOL in the chosen power weighs 20 mg, the capsular tension ring weighs 1 mg, and the 9.5-mm ArtificialIris weighs 30 mg, for a total implanted weight of 51 mg—well below the natural weight of the crystalline lens. Therefore, the zonules should not be stressed.
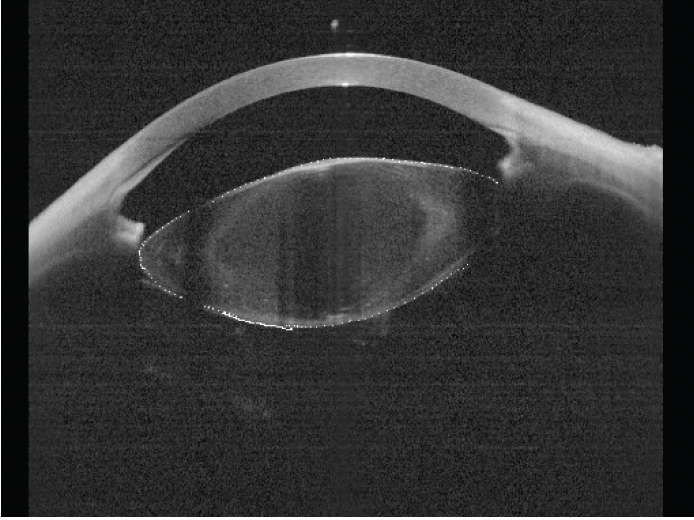
Figure 3. Professor Goldblum outlined the lens capsule so that Haag-Streit could calculate the diameter.
POSTOPERATIVE RESULT
Immediately after surgery, the patient experienced ocular hypertension with a peak of 28 mm Hg that was managed with a short-term prescription for IOP-lowering drops. She regained her normal visual acuity of 0.3 (preoperative 0.1), which she was happy with.
Several weeks after cataract surgery and ArtificialIris implantation, the patient returned for a cosmetic bilateral ptosis procedure. Figure 4 shows the final result.
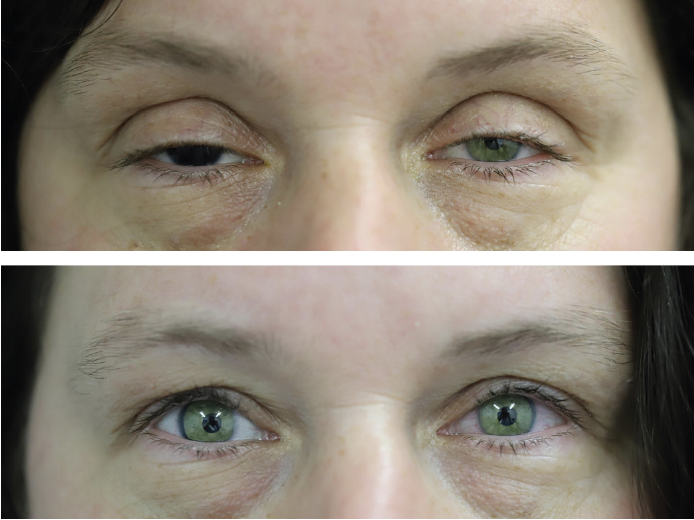
Figure 4. The final postoperative result after bilateral ptosis.
CONCLUSION
Working with Haag-Streit in a unique way to help to customize the surgical procedure for this patient with congenital aniridia was a rewarding experience. Trephinating the artificial iris in the capsular bag avoided having to implant the device in the sulcus as well as touching the ciliary structures. In the end, this approach decreased the risk for glaucoma and inflammation.