

Patients who present for a cataract surgery evaluation have often done their own research and are aware of basic options. For many, the focus is on spectacle independence without compromises. Surgical planning, especially when a premium IOL is involved, is crucial.
Today, we need more than axial length and keratometry to help our patients decide what type of IOL is best for them. The Cataract Suite of the Eyestar 900 (Haag-Streit) allows a comprehensive evaluation of almost any type of cataract, which can help surgeons review the suitability for a specific IOL and improve surgical planning and postoperative outcomes. Additionally, visual simulation can also be used to educate patients interactively about their condition and treatment options.
CLINICAL VALUE
Using swept-source OCT, the Eyestar 900 can penetrate almost any cataract to provide highly accurate axial measurements of the entire eye, from the cornea to the retina. There is also standard dual-zone reflective keratometry for highly accurate corneal power, 7.5 mm diameter topography with the Cataract Suite, and up to a 12 mm diameter with the Anterior Chamber Suite software option that incorporates the anterior and posterior corneal surfaces. B-scan imaging of the anterior chamber also includes the lens and an accurate assessment of tilt and decentration. These measurements allow the user to identify anatomical anomalies that may interfere with the surgical plan.
Other advantages of the Eyestar 900’s Cataract Suite add to the device’s clinical value, including a Zernike analysis and vision simulation. These will be the focus of this article, along with best practices for topography.
TOPOGRAPHY
The topographic maps of the Eyestar 900’s Cataract Suite cover a 7.5-mm zone. The Anterior Chamber Suite incorporates data from the anterior and the posterior cornea and covers up to 12 mm.
Keratometry is a crucial feature in biometry, and the Eyestar can approach this in several ways. The first is standard keratometry based on an ellipsoid with flat and steep meridians perpendicular to one another. The Eyestar also uses zone-based keratometry, which incorporates up to four meridians—two steep and two flat and completely independent in terms of their orientation and power.
From a clinical perspective, zone-based keratometry allows surgeons to screen for signs of corneal pathologies that may limit visual potential. This form of keratometry can be used to identify regular and symmetrical astigmatism and validate standard reflective and simulated keratometry. The extra validation is especially helpful when considering candidates for toric and multifocal IOLs (Figure 1).
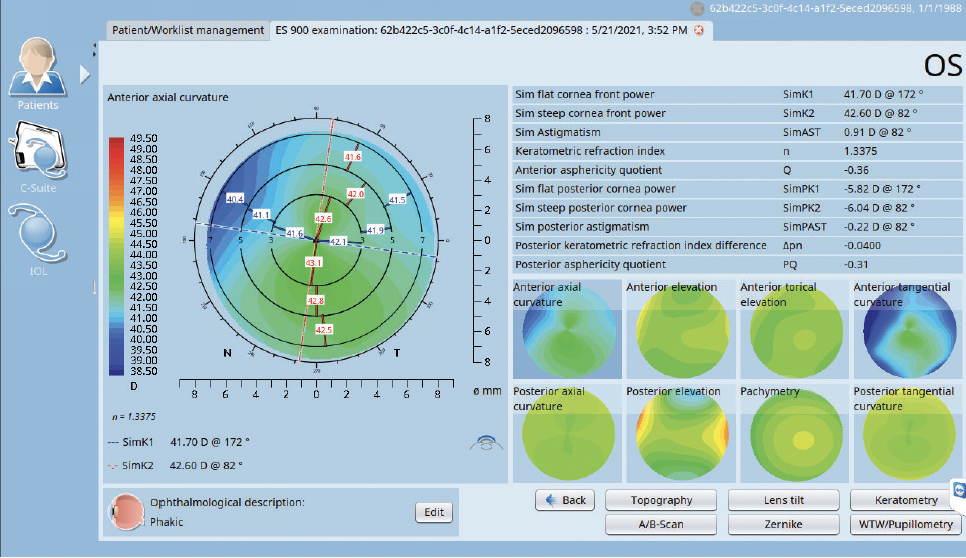
Figure 1. The bowtie on topography illustrates some bending and asymmetry in the astigmatism. Zone-based keratometry, however, can clearly quantify and depict the imperfections of the astigmatism, helping the surgeon in the decision-making process for the optimal IOL.
ZERNIKE ANALYSIS
Together, the Zernike polynomials are a valuable clinical tool used to describe wavefront aberrations of the cornea or the lens from an ideal shape that results in a loss of image contrast. The presence of third- and fourth-order aberrations can significantly impact the quality of vision due to a loss of contrast sensitivity. From the perspective of the ophthalmic surgeon, the third-order aberration coma is a form of irregular astigmatism that produces variable amounts of image duplication and displacement. Spherical aberration is a fourth-order aberration that produces a characteristic image, halo and glare. The mathematical construct of the Zernike polynomials qualifies these aberrations into values measured in microns, which can also be used for image sumulation and as part of our preoperative evaluation.
The Zernike wavefront analysis by the Eyestar 900 is highly useful for determining how individual and groups of aberrations impact visual quality. This feature can quantify the full range of aberrations, which can be converted into an easily understoond image simulation. Removing individual aberrations from an image simulation can be a powerful tool for demonstrating how correcting corneal astigmatism using a toric IOL improves vision. Removing all aberrations is an elegant way to demonstrate how the loss of contrast from a highly irregular corneal surface can be dramatically corrected by a rigid gas permeable or scleral contact lens.
For patients who have previously undergone refractive surgery (eg, radial keratotomy, LASIK, PRK), image simulation is a useful way to show how an increase in spherical aberration and coma impacts visual quality. Image simulation can also show why certain options, such as a multifocal IOL, may not be a good choice.
Reviewing the wavefront analysis provides meaningful talking points when discussing IOL selection. It can help facilitate patient discussion as to why a certain IOL is better suited to them as an individual. The Zernike wavefront analysis also produces individual coefficients at different pupil sizes so that patients can get a feel for their vision in certain lighting conditions (Figure 2).
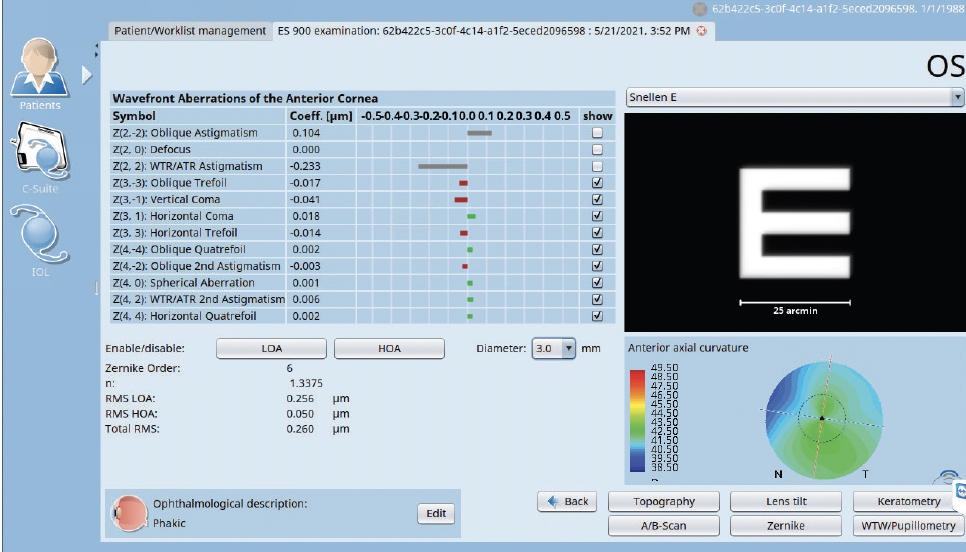
Figure 2. The Zernike wavefront analysis paired with an image simulation and a display of the anterior curvature map provides the eye care specialist with a versatile tool that can be used to demonstrate to the patient the improvement in visual quality following toric IOL placement. The influence of changing ambient light conditions may also be shown by adjusting the pupil diameter in real-time.