

Today, minimizing or even eliminating preexisting astigmatism at the time of cataract surgery is one crucial component of achieving our patients’ expectations. Luckily, cataract surgeons have several options for correcting astigmatism during surgery, including toric IOLs and manual and laser-assisted limbal relaxing incisions. In my practice, the majority of patients who come in seeking cataract surgery and have astigmatism of up to 1.00 D receive a toric IOL. For the past year, the lens I choose has always been the Precizon Toric IOL (OPHTEC), and I intend to continue using it, as it is the most tolerant of misalignment and can provide patients with at least 1 additional line of uncorrected vision compared to the other toric IOLs I have used.
WHY A TORIC?
It is important to correct preexisting astigmatism at the time of cataract surgery because, first, patients tend to be the happiest postoperatively when their cylinder is corrected. Second, I have noticed that the subjective and objective outcomes will be better than they would have been had a toric IOL not been elected.
WHICH DESIGN?
With so many toric IOLs available in Europe right now, selecting the right one might take some time. I have experience with several toric lens models, but I have found the Precizon Toric IOL to be the best option for my patients for several reasons.
Reason No. 1: Stability. The biggest benefit to this lens and the way it differentiates itself from other toric IOLs is with its unique Transitional Conic Toric surface. It is common knowledge that, for every degree an IOL is rotated from the intended axis of implantation, a toric lens will lose 3% of its effectiveness in treating astigmatism. However, the Precizon is more tolerant of misalignment due to this Transitional Conic Toric surface,1-4 which blends into the aspheric surface of all meridians of the IOL and leads to a broader toric surface, an extended depth of focus, and better alignment of the toric surface with the patient’s astigmatism, even when slightly misaligned.
In one study of 40 eyes of 27 patients with corneal astigmatism greater than 1.00 D, Vale et al found that the mean IOL rotation with the Precizon was 2.43 ±1.55º, and none of the IOLs required realignment postoperatively. At the last follow-up visit, mean refractive spherical equivalent decreased from -3.35 ±3.10 D to -0.02 ± 0.30 D (P = .110), and 97.5% of eyes were within ±0.50 D of emmetropia.1 Likewise, in a study evaluating the rotational stability of four aspheric toric IOLs (transitional conic toric, bitoric, posterior toric surface, and anterior toric surface) using an optical bench system,2 the Precizon outperformed two of the other three torics (posterior and anterior toric surface IOLs) in terms of rotation-induced deterioration when each was decentered by 1 mm and the contrast reduction rate was 17.6 cycles per degree (5.1% Precizon vs 3.1% bitoric, 12.2% posterior toric surface, and 15.8% anterior toric surface); when the contrast reduction rate was 0.5, rotation-induced deterioration required a much higher rotation in the Precizon Toric IOL than in the other lenses in the study.
Although the Precizon tends to provide similar results in terms of rotational stability at 1 month postoperatively, according to a study by Mertens,3 the lens performs significantly better in astigmatism correction and does not show as much sensitivity to misalignment as another toric IOL (Lentis Toric; Oculentis). Dr. Mertens’ results highlight that the transitional conic surface of the Precizon provides greater tolerance for misalignment and greater chance for improved outcomes (Figure 1).
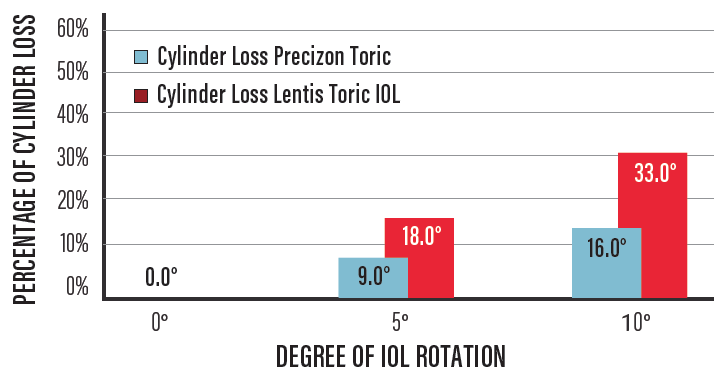
Figure 1. Precizon Toric vs Lentis Toric IOL: Cylinder loss per degree of rotation.
I have had similar experiences to those described by others1-5 in the little more than 1 year that I have been implanting the Precizon. In the more than 100 eyes that I have used the Precizon, I have only had to reposition the lens once.
Another element contributing to the stability of the Precizon is the lens’ haptics. Designed to ensure that the space between the inner haptic of the lens stays open with compression down to 9 mm, the haptics create a fibrosis anchor to not only enhance the stability of the lens but also to reduce late postoperative rotation. Further, the haptics are also offset in shape, enabling the lens to adhere to the posterior capsule, prevent early postoperative rotation, and reduce the risk for posterior capsular opacification.
Reason No. 2: The lens has an aberration-neutral design, meaning fewer spherical aberrations and fewer visual side effects. The Precizon Toric IOL has an aspherical cylinder and an aspherical anterior side, which results in an aberration-neutral design. This contrasts with lenses that have a conventional spheric lens design, in which spherical aberration results due to the dioptric power in the periphery of the lens being different from the dioptric power on the optical axis. Such aberrations influence contrast sensitivity and depth of focus and can result in unwanted visual side effects, like halos and glare.
In the study by Kim et al,1,2 it was also determined that aberration-free IOLs, such as the Precizon, provided patients with better contrast sensitivity than IOLs with negative asphericity. Also, the Precizon provided better image contrast according to the degree of rotation (Figure 2).
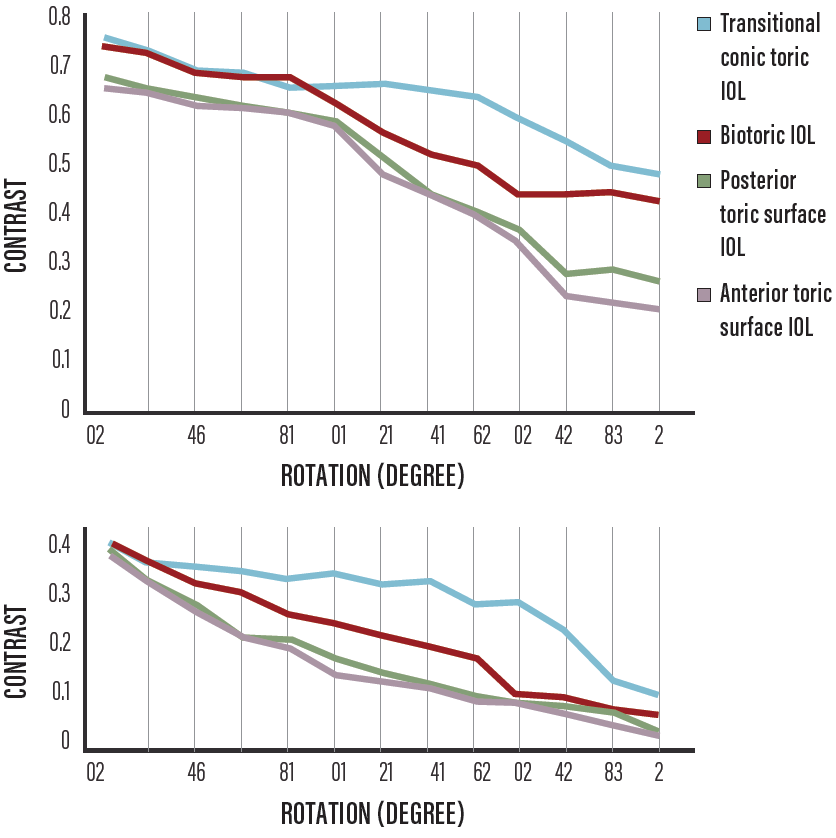
Figure 2. Image contrast according to degree of IOL rotation with the 4-mm pupil at 17.6 cpd (top) and 35.2 cpd (bottom).
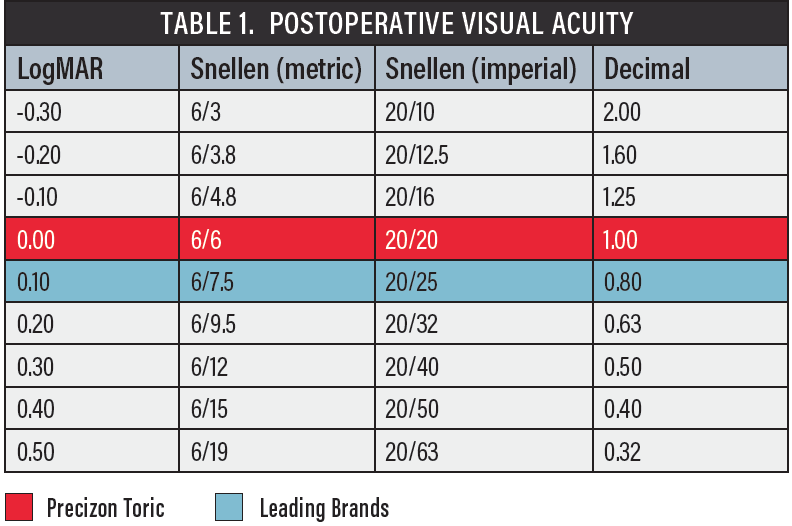
Reason No. 3: It provides at least 1 additional line of UCVA compared with other leading toric IOLs. According to two analyses by Ferreira and colleagues,4,5 the Precizon can effectively provide patients with better UCVA compared to leading toric brands (Table 1). I have also found similar results in my own experience. Generally speaking, patients achieve excellent visual acuity and quality, and they are extremely happy with their results.
OTHER OBSERVATIONS
In every case, I combine the Precizon Toric lens with laser cataract surgery. Using this approach, what we have found is that patients experience very stable postoperative effects over 12 months. There simply is minimal to no rotation in the capsular bag postoperatively.
I also like this lens because I can easily implant it through a 2.4-mm incision, which can help to minimize surgically induced astigmatism.
CONCLUSION
The Transitional Conic Toric surface of the Precizon Toric IOL is beneficial for many reasons, the most important of which is that it is more tolerant of misalignment. This can lead to better postoperative results, an extended depth of focus, and even additional lines of uncorrected vision when compared to other toric IOLs available today.
Precizon’s Transitional Conic Toric Optic was recently granted a US patent.
1. Vale C, Menezes C, Firmino-Machado J, Rodrigues P, et al. Astigmatism management in cataract surgery with Precizon toric intraocular lens: a prospective study. Clinical Ophthalmol. 2016;19.
2. Kim MJ, Yoo YS, Joo CK, et al. Evaluation of optical performance of 4 aspheric toric intraocular lenses using an optical bench system: Influence of pupil size, decentration, and rotation. J Cataract Refract Surg. 2015;41(10):2274-2282.
3. Mertens E. Evaluation of a new toric IOL optic by means of intraoperative wavefront aberrometry (ORA System): the effect of IOL misalignment on cylinder reduction. Paper presented at: the 2014 European Society of Cataract and Refractive Surgeons meeting; September 13-17, 2014; London.
4. Ferreira TB. Visual and optical outcomes of a new monofocal toric intraocular lens. Paper presented at: the 2015 European Society of Cataract and Refractive Surgeons meeting; September 5-9, 2015; Barcelona, Spain.
5. Ferreira TB, Almeida A. Comparison of the visual outcomes and OPD-Scan results of AMO Tecnis Toric and Alcon Acrysof IQ toric intraocular lens. J Refract Surg. 2012;28(8):551-555.



