
 Correction of astigmatism at the time of cataract surgery has become increasingly more important as our patients continue to demand more from their surgical procedure than simple crystalline lens removal. Today, we can offer patients a variety of options to managing their astigmatism, including adjusting the axis of the primary phaco incision, placing additional limbal relaxing incisions, and implanting a toric IOL.
While all aim to correct the astigmatism, some are more successful than others. Toric IOLs, for instance, can successfully and accurately address astigmatism; however, most toric IOL calculators are based on anterior keratometry measurements alone and do not take the posterior cornea into account. As we know from Koch et al,1 posterior corneal astigmatism significantly affects the total corneal cylinder, and therefore, when a standard toric IOL calculator is used, an against-the-rule error.
As a means to solve this problem, Adi Abulafia, MD, and Douglas D. Koch, MD, developed the Abulafia-Koch formula for toric IOL power calculation (described in detail on pages 22 and 23). PhysIOL has now made this formula commercially available, and we have plans to introduce it at our clinic.
Memira is a Scandinavian chain of 40 private refractive surgery clinics. We perform 18,000 refractive surgeries annually, and to date, we have implanted more than 30,000 FineVision IOLs, including the FineVision trifocal toric. In the past few years, almost 30% of the IOLs we implant have been toric. In order to calculate IOL power with the FineVision toric, for the past several years we have taken the expected effect from the posterior cornea into account manually. The refractive astigmatism outcomes are therefore good, yet the improvement in the calculator to incorporate the Abulafia-Koch formula will perhaps enhance the results even more. The main advantage to us is that the formula is incorporated into the calculator, so that we no longer need to adjust manually.
Correction of astigmatism at the time of cataract surgery has become increasingly more important as our patients continue to demand more from their surgical procedure than simple crystalline lens removal. Today, we can offer patients a variety of options to managing their astigmatism, including adjusting the axis of the primary phaco incision, placing additional limbal relaxing incisions, and implanting a toric IOL.
While all aim to correct the astigmatism, some are more successful than others. Toric IOLs, for instance, can successfully and accurately address astigmatism; however, most toric IOL calculators are based on anterior keratometry measurements alone and do not take the posterior cornea into account. As we know from Koch et al,1 posterior corneal astigmatism significantly affects the total corneal cylinder, and therefore, when a standard toric IOL calculator is used, an against-the-rule error.
As a means to solve this problem, Adi Abulafia, MD, and Douglas D. Koch, MD, developed the Abulafia-Koch formula for toric IOL power calculation (described in detail on pages 22 and 23). PhysIOL has now made this formula commercially available, and we have plans to introduce it at our clinic.
Memira is a Scandinavian chain of 40 private refractive surgery clinics. We perform 18,000 refractive surgeries annually, and to date, we have implanted more than 30,000 FineVision IOLs, including the FineVision trifocal toric. In the past few years, almost 30% of the IOLs we implant have been toric. In order to calculate IOL power with the FineVision toric, for the past several years we have taken the expected effect from the posterior cornea into account manually. The refractive astigmatism outcomes are therefore good, yet the improvement in the calculator to incorporate the Abulafia-Koch formula will perhaps enhance the results even more. The main advantage to us is that the formula is incorporated into the calculator, so that we no longer need to adjust manually.
STUDY OF REFRACTIVE RESULTS
Before implementing the Abulafia-Koch formula at our clinics, we first rode tested it on historical data. Reviewing 653 eyes implanted with a trifocal toric IOL in our Norwegian clinics, we looked at three things: (1) the predicted residual astigmatism with the former PhysIOL toric calculator, (2) the predicted residual astigmatism with the current PhysIOL toric calculator with the Abulafia-Koch formula, and (3) the astigmatic outcomes at 3 months postoperatively. We then compared the actual outcomes with the predicted values from both calculators.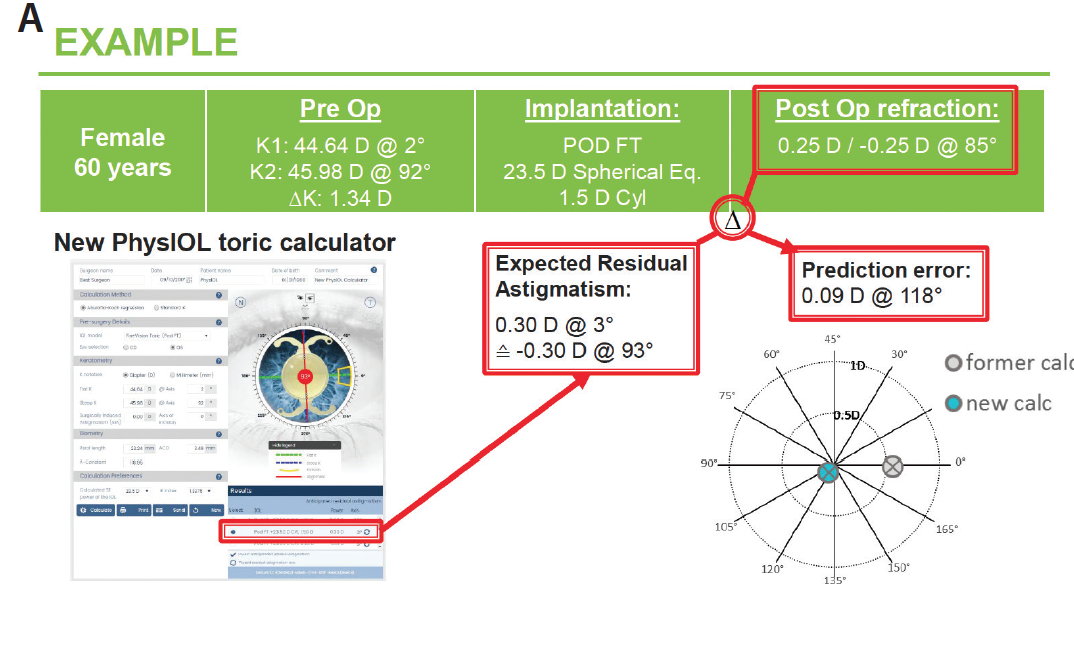
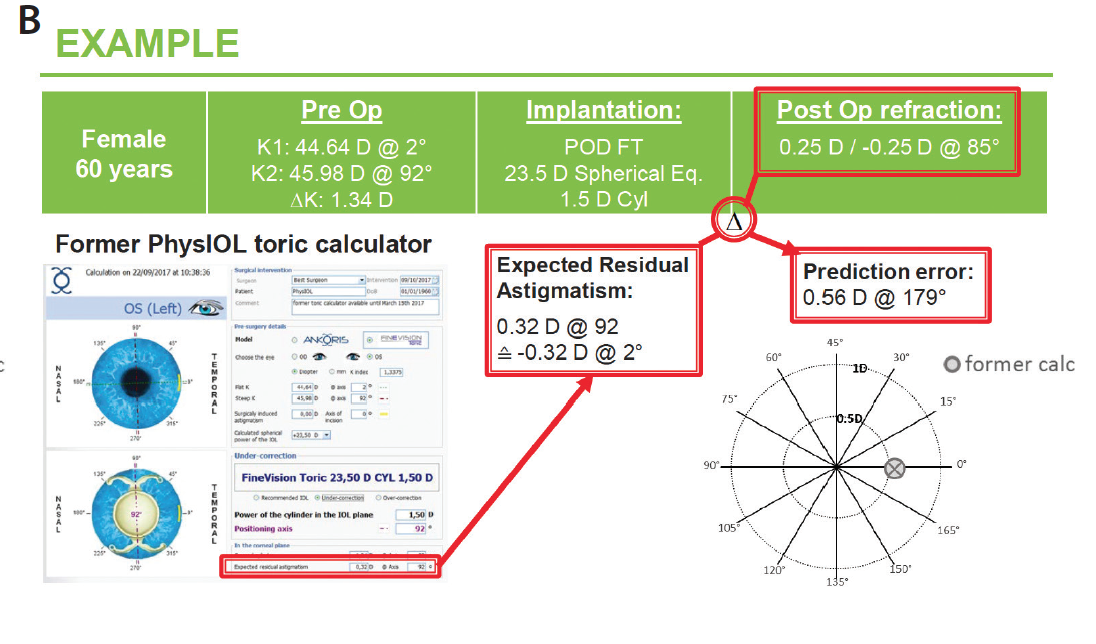
Figure 1. Expected residual astigmatism and prediction error with the former PhysIOL toric calculator (A) and the current calculator with the Abulafia-Koch formula (B).
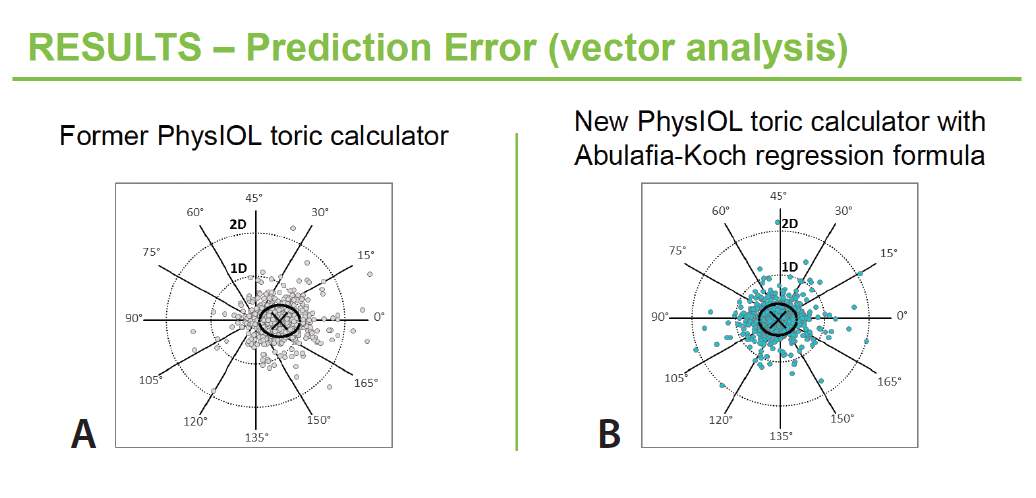
Figure 2. Prediction errors with the former PhysIOL toric calculator (A) and the current calculator with the Abulafia-Koch formula (B).
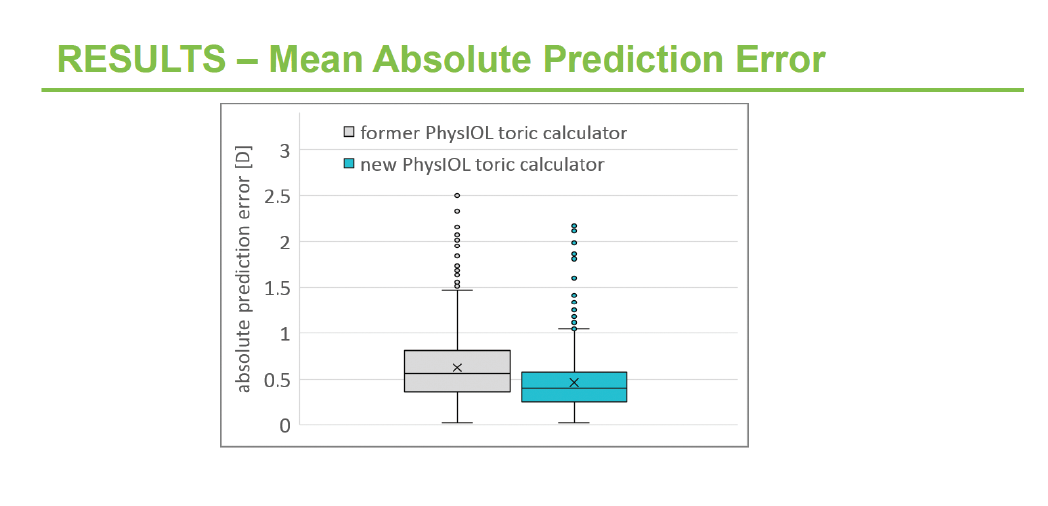
Figure 3. Mean absolute prediction errors with the former PhysIOL toric calculator (gray) and the current calculator with the Abulafia-Koch formula (teal).
