
Sponsored By


Small incision lenticule extraction, or SMILE, has become a widely accepted method of laser vision correction, and we are very close to 1 million procedures completed worldwide. Even though we do not know the exact date the first SMILE surgery was performed, we know it was some time in April 2007. Something I can remember, though, was the day that I performed the first iteration of the SMILE procedure, femtosecond lenticule extraction, or FLEx, for the first time. This was May 3, 2006.
Once FLEx was an established technique, Marcus Blum, MD, and I started to reduce the incision size required of the procedure. The first SMILE had two opposite incisions that were each 5 mm. It was Rupal Shah, MD, who then made the next step in the progression of SMILE by performing it through a single incision. Since this time, the technique has continued to advance dramatically. Now that SMILE has been approved by the US FDA, we can say that the the procedure is no embraced by the entire corneal refractive surgery community.
TRACKING THE FIRST PATIENTS
Not only have 5-year results of both SMILE and FLEx been published by our group,1 but peer-reviewed 4-year results with the current VisuMax 500 kHz-laser (ZEISS) have also been published.2 Several 3-year studies from us and other investigators are also available.3-5
SMILE has become a hot topic; in a recent PubMed search, I found 280 citations on SMILE, including five major reviews6 and three large meta-analyses.7-9 Moreover, two books, one in Chinese and one in English, are already available, and another book in English and Spanish is due to be released. Dr. Blum and I are privileged to be the first in the world to perform SMILE surgery, and we are currently preparing a 10-year follow-up study of the first patients treated in 2007.
We were also able to track some of the patients who had undergone FLEx in Marburg, Germany, 10 to 11 years ago. The most impressive outcome was that BCVA has not deteriorated (Figure 1). In terms of stability (Figure 2), 1-month and 10-year mean spherical equivalent was -0.58 and -0.70 D, respectively. The remarkable stability of the first five eyes ever treated raise hopes that our 10-year SMILE study will also provide similarly good long-term results.
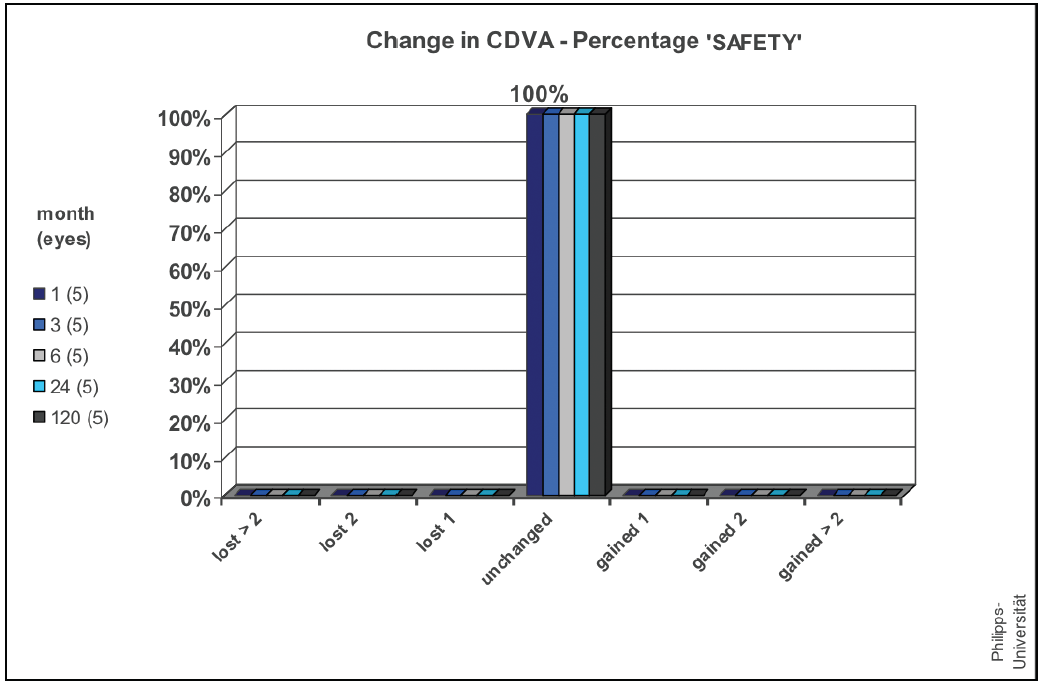
Figure 1. BCVA at 1, 3, 6, 24, and 120 months postoperative.
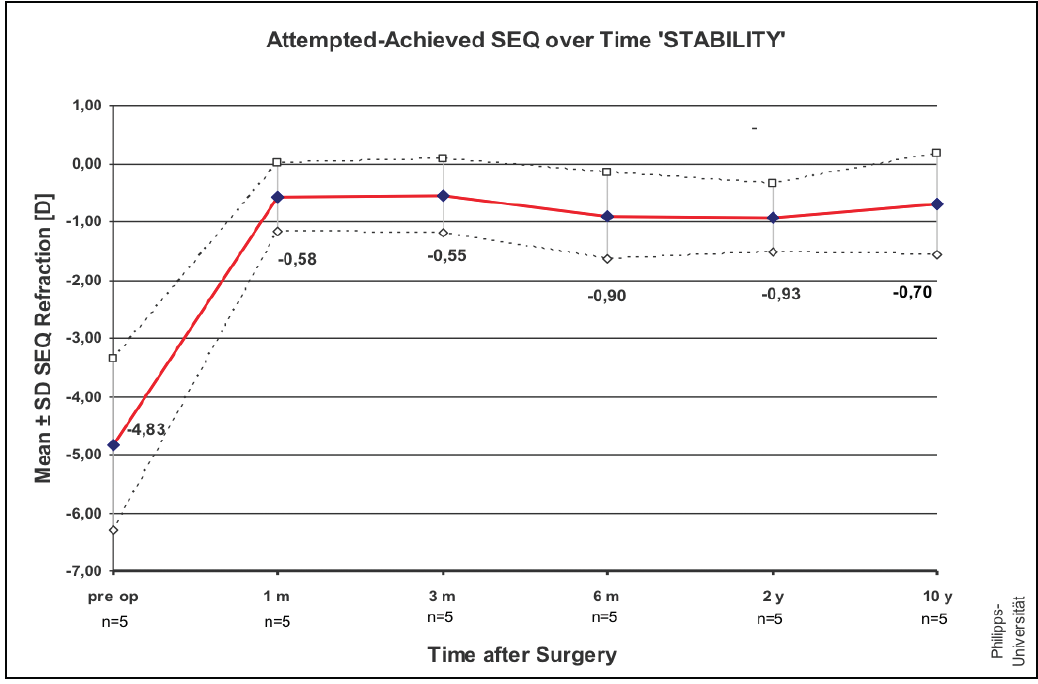
Figure 2. Mean spherical equivalent at 1, 3, 6, and 24 months and 10 years.
A LONG-LASTING EFFECT
In my opinion, several considerations will have a long-lasting effect on the refractive market. There is, for instance, no doubt that SMILE, when performed through a true small incision size between 2 and 3 mm, has less destructible effect on corneal sensation in the short-term.10 Further, theoretical, experimental and clinical studies for high myopia have shown that SMILE has less short- and long-term weakening effects on corneal biomechanics compared with other laser vision correction procedures.11
The centration issue that has been discussed for a considerable time is no longer relevant since several studies showed that patient’s self-centration yields better results than surgeon-controlled eye-tracker centration with excimer laser ablations.12-14
The issue of cyclotorsion has at least been partially resolved by an idea proposed by several groups of surgeons, including Ivarsen and Hjordtal, of Arhus, Denmark, who have provided guidance on how to mark the cornea and rotate the suction cone according to the marks. Although this is controversial, Dr. Ivarsen’s method has proved to be extremely effective in daily routine practice as shown by Brar and Ganesh.15 Of course, an automatic cyclotorsion and adjustment control would further increase the acceptance of SMILE surgery.
Another major step was an investigator-initiated trial, led by Kishore Raj Pradhan, MD, to introduce hyperopic SMILE. At the same time, our group had successfully finished a hyperopic FLEx study, and the final results were released at the beginning of 2017. We are in the process of publication now.
Energy management with the VisuMax femtosecond laser has allowed surgeons to expand the capabilities of SMILE and has also improved the cutting quality and shortened the surgical time. Helpful rescue software included in the laser aids novice surgeons in making the right decisions in critical situations, such as suction loss. Last but not least, the idea of lenticule implantation and autotransplantation has been studied by several investigators, and it has proved to be useful in certain special situations.16
A FIRST-CHOICE PROCEDURE
Taken together, there is no wonder that SMILE is on the way to becoming a first-choice refractive procedure, in particular for higher myopia and in young patients. At the same time, it does not mean in any way that femtosecond LASIK is not a good procedure. It has some advantages and disadvantages compared to SMILE and should be considered as one of the assets for safe, patient-oriented, comfortable refractive surgery. Together these procedures have the potential to hopefully drive the refractive market to new heights.
1. Blum M, Taeubig K, Gruhn C, Sekundo W, Kunert KS. Five-year results of small incision lenticule extraction (ReLEx SMILE). Br J Ophthalmol. 2016;100(9):1192-1195.
2. Han T, Zheng K, Chen Y, Gao Y, He L, Zhou X. Four-year observation of predictability and stability of small incision lenticule extraction. BMC Ophthalmol. 2016;16(1):149.
3. Messerschmidt-Roth A, Sekundo W, Lazaridis A, Schulze S. Three years follow-up study after refractive small incision lenticule extraction (SMILE) using 500 kHz femtosecond laser in “fast mode.” Klin Monbl Augenheilkd. 2017;234(1):102-108.
4. Pedersen IB, Ivarsen A, Hjortdal J. Three-year results of small incision lenticule extraction for high myopia: Refractive outcomes and aberrations. J Refract Surg. 2015;31(11):719-724.
5. Han T, Zhao J, Shen Y, Chen Y, Tian M, Zhou X. A three-year observation of corneal backscatter after small incision lenticule extraction (SMILE). J Refract Surg. 2017;33(6):377-382.
6. Reinstein DL, Morshirfar Shen Z et al. PLOS One 2016.
7. Wang JS, Xie HT, Jia Y, Zhang MC. Small-incision lenticule extraction versus femtosecond lenticule extraction for myopic: a systematic review and meta-analysis. Int J Ophthalmol. 2017;10(1):115-121.
8. Ag˘ca A, Demirok A, Yıldırım Y, Demircan A, Yas¸a D, Yes¸ilkaya C, Perente I˙, Tas¸kapılı M. Refractive lenticule extraction (ReLEx) through a small incision (SMILE) for correction of myopia and myopic astigmatism: current perspectives. Clin Ophthalmol. 2016;10:1905-1912.
9. Shen Z, Shi K, Yu Y, Yu X, Lin Y, Yao K. Small incision lenticule extraction (SMILE) versus femtosecond laser-assisted in situ keratomileusis (FS-LASIK) for myopia: A systematic review and meta-analysis. PLoS One. 2016;11(7):e0158176.
10. Cai WT, Liu QY, Ren CD, Wei QQ, Liu JL, Wang QY, Du YR, He MM, Yu J. Dry eye and corneal sensitivity after small incision lenticule extraction and femtosecond laser-assisted in situ keratomileusis: a meta-analysis. Int J Ophthalmol. 2017;10(4):632-638.
11. Spiru B, Kling S, Hafezi F, Sekundo W. Biomechanical differences between femtosecond lenticule extraction (FLEx) and small incision lenticule extraction (SmILE) tested by 2D-extensometry in ex vivo porcine eyes. Invest Ophthalmol Vis Sci. 2017;58(5):2591-2595.
12. Lazaridis A, Droutsas K, Sekundo W. Topographic analysis of the centration of the treatment zone after SMILE for myopia and comparison to FS-LASIK: subjective versus objective alignment. J Refract Surg. 2014;30(10):680-686.
13. Reinstein DZ, Pradhan KR, Carp GI, Archer TJ, Gobbe M, Sekundo W, Khan R, Citron K, Dhungana P. Small incision lenticule extraction (SMILE) for hyperopia: Optical zone centration. J Refract Surg. 2017;33(3):150-156.
14. Reinstein DZ, Gobbe M, Gobbe L, Archer TJ, Carp GI. Optical zone centration accuracy using corneal fixation-based SMILE compared to eye tracker-based femtosecond laser-assisted LASIK for myopia. J Refract Surg. 2015;31(9):586-592.
15. Brar S. Paper presented at: the European Refractive Symposium; June 2016; Potsdam, Germany.
16. Ganesh S, Brar S, Rao PA. Cryopreservation of extracted corneal lenticules after small incision lenticule extraction for potential use in human subjects. Cornea. 2014;33(12):1355-1362.
