
Sponsored by Carl Zeiss

BY FLORIAN KRETZ, FEBO
Ahaus, Germany
Dr. Florian Kretz is the CEO of Eyedoctors Gerl, Kretz & Collegues, Ahaus-Greven-Ochtrup-Raesfeld-Rhede-Rheine-Stadtlohn- Steinfurt, Germany, and Consultant at the International Vision Correction Research Centre & David J Apple Laboratory in Heidelberg, Germany
Case History
A 77-year-old male presented complaining of severe glare during nighttime driving due to a posterior subcapsular cataract. The patient is demanding of his intermediate and distance visual acuity as he is not a typical book reader but instead reads on his smart phone, tablet, or the dashboard on his vehicle. He also does wood craft work in his spare time. He was typically seeing at distances farther than 50 cm.
Preoperative Assessment
The patient underwent an evaluation from our IOL counselors, which included a detailed anamnesis about his preferred distances in performing near and intermediate tasks during daily routine. Next, the patient’s eyes were measured using SWEPT Source Optical CoherenceTomography (OCT) technology (IOLMaster 700; Carl Zeiss Meditec AG) and anterior segment tomography (Pentacam; Oculus) as well as a macular screening with the SWEPT Source OCT (Cirrus 5000, Carl Zeiss Meditec AG). Based on his responses to the anamnesis, it was clear that the patient was focused on optimal distance and intermediate vision, especially considering he used to be a driver. I then counseled the patient on IOL possibilities based on the pros and cons of each model. I recommended the AT LARA 829MP (Carl Zeiss Meditec AG) because of its spherical & chromatic aberration correction (Figure 1), which gives better distance vision than other multifocal lenses and also provides less visual disturbances, such as halo and glare due to its enhanced depth of focus optical pattern.
Fig. 1 ZEISS AT LARA 829MP
The spherical equivalent (SE) of the IOL was 21.0 OD and 20.5 OS. Target refraction was -0.21 D OD and -0.02 D OS. Using the Haigis IOL formula, induced astigmatism was 0.5 OU with a 90° incision OU. K1 and K2 readings were 7.59 mm and 7.55 mm OD, respectively, and 7.55mm and 7.49 mm OS, respectively. His objective and subjective spherical refractions were 1.75 D OD and 4.00 D OS. Preoperative cylinders were -1.75 D OD and -4.00 D OS. Preoperative SE was 0.875 D OD and 2 D OS.
Cataract Surgery and IOL Implantation
For the surgical process, I made two 1-mm side-cut incisions followed by a 2-mm main incision on the steep axis. I filled the anterior chamber with cohesive viscoelastic and performed the capsulorhexis with a 23-gauge microforceps. Next, I performed hydro-dissection and hydrodeliniation. I facilitated the cataract removal with a chop and stop technique. Afterward, I performed a bimanual cortex removal and capsular bag polish, removing the remaining remnants of the lens and polishing the anterior and posterior capsule. I implanted the AT LARA 829MP with the irrigation port through the sideport using balanced salt solution irrigation only so that I didn’t need to remove any viscoelastic after implantation. Afterward, I hydrated the side ports and washed the anterior chamber with Cefuroxom. Overall, the procedure took 6 minutes to complete per eye.
Near, Intermediate, And Far Visual Outcomes
I had the patient return at 1 day, 1 week, and 3 months postoperatively. At the 3-month postoperative visit, the patient’s postoperative SE was -0.125 D OD and -0.75 OS. His uncorrected distance visual acuity (CDVA) logMAR value was 0 OD and 0.15 OS. His distance corrected intermediate visual acuity (DCIVA) was 0.2 OU at 90 cm, 0.2 OU at 80 cm, and 0.2 OU at 60 cm. Distance corrected near visual acuity (DCNVA) was 0.5 OU at 40 cm. During the halo and glare assessment the patient didn’t experience any photic phenomena (Figures 2). The postoperative McAlinden patient satisfaction questionnaire only showed “no” as an answer for possible side effects.
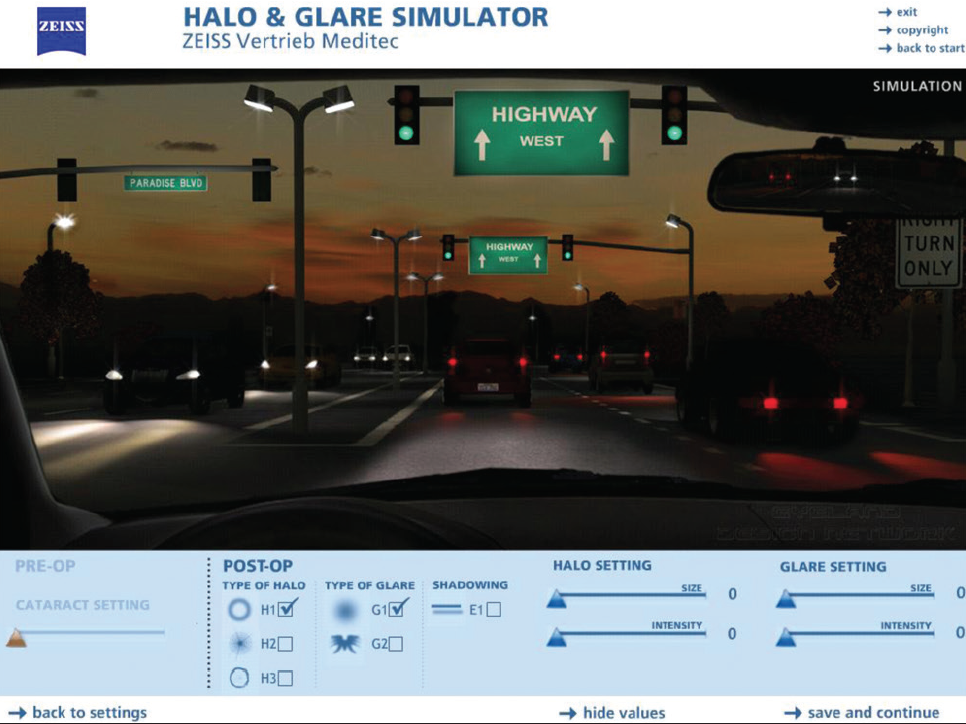
Fig. 2 Halos & Glare Simulation Tool
The binocular defocus curve analysis showed a visual acuity of ³ 0.3 logMAR in a range of -2.5 D to +1.5 D and of ³ 0.1 logMAR in a range of -1.5 D to +0.5 D. Those results and absence of visual side effects, especially for different intermediate distances ranging from 60 to 90cm were the main reason for the patient’s high satisfaction.
Discussion
The AT LARA 829MP from ZEISS is one of few enhanced depth of focus (EDoF) IOLs based on a diffractive optical pattern. The additional correction for chromatic aberration enhances the distance visual acuity outcomes by maintaining a wide range of vision for intermediate tasks. For patients who have their main focus for distance and intermediate vision from 60 cm on without accepting a blended vision approach, the AT LARA 829MP is my first choice.
