
Sponsored by Oculentis

Over the past decade, we have seen a rise in the popularity of selecting multifocal IOLs for cataract surgery as well as for refractive lens exchange procedures. This now common alternative to monofocal IOLs in patients seeking spectacle independence can provide exceptional near and distance UCVA and quality intermediate UCVA; however, multifocal IOLs are not without side effects, such as reduced contrast sensitivity, increased visual aberrations, halos, glare, and negative dysphotopsias (Figure 1).
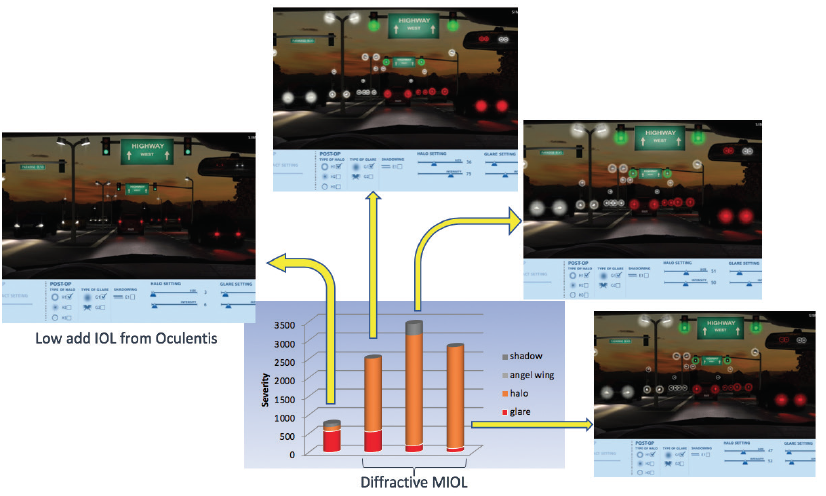
Source: Patrick Versace, MD, case report IOL exchange presented at the Oculentis International User Meeting 2018 in Vienna
Figure 1. Simulation of halos and glare with multifocal IOLs.
It is our observation and that of others that the main determinant of unwanted visual phenomena is lens design and its optical parameters. Lens position and decentration may also contribute and necessitate lens explantation/exchange. Even more rare causes include IOL opacification, endothelial cell damage, chronic uveitis, and capsular phimosis. Although many patient complaints, regardless of the cause, can be managed with IOL repositioning, spectacles, contact lenses, or an enhancement procedure, in some cases an IOL exchange may be necessary.
BACKGROUND
When looking at the trends in IOL exchange from 2007 to 2011, Jones et al1 determined that 46% of lenses were exchanged due to dislocation or incorrect position, 23% due to incorrect IOL power, 21% due to patient dissatisfaction, and 7% due to lens opacification. Of the dissatisfied patients, 42% had undesired visual acuity even without symptoms of glare or optical aberrations.
Happily, when the IOL was exchanged for another lens, the mean logMAR BCVA improved significantly (P < .001) in the majority of cases. That is, 88% of eyes were 20/40 or better, with no vision-threatening complications in any procedure.
Surgeons should rely on their own expertise and the tools that they have available to them when deciding on how to best manage the unhappy patient. In this article, I present a recent case in which the patient was unhappy after presbyopia-correcting IOL implantation and discuss my reasons for deciding on an IOL exchange procedure with the LENTIS Comfort IOL (Oculentis).
The Comfort IOL is based on the LENTIS Mplus technology (Oculentis), a refractive, segmental asymmetric IOL designed to minimize the interfaces between near and far vision—thus optimizing visual quality with reduced unwanted visual phenomena. This has proven to be a successful strategy with high patient satisfaction and minimal undesirable visual effects while also providing patients with a functional range of near, intermediate, and distance vision. The Comfort version of the IOL has less near add (1.50 D) and behaves as an extended depth of focus (EDOF) IOL.
CASE PRESENTATION
I was recently referred a patient who was unhappy with his vision in an eye that had been implanted with a small-aperture presbyopia-correcting IOL (IC8, AcuFocos). In his late 50s, this patient was a very active hyperopic presbyope who had originally sought surgery to reduce his need for spectacles. His lens implant surgery was perfect and without complication; however, he was unhappy with the quality of his vision and complained of halos, glare, and lack of brightness.
On examination, he was noted to have a large pupil, a well-positioned IOL, and dense posterior capsular opacification (PCO) (Figure 2). After some discussion, we agreed to proceed with IOL exchange. I did not want to open the posterior capsule because his visual symptoms predated the onset of PCO and a lens exchange procedure would become more complex with an open posterior chamber. We selected the LENTIS Comfort (1.50 D near add), as this lens would provide the patient with a functional range of near, intermediate, and far vision with minimal chance of any unwanted visual phenomena.
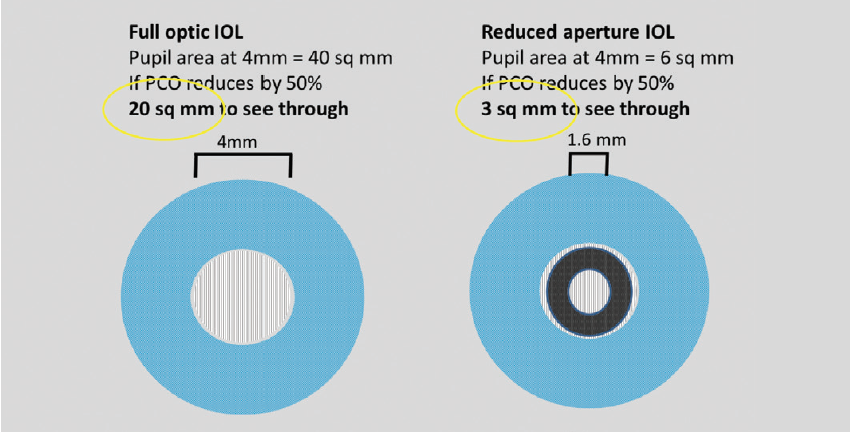
Figure 2. PCO can cause a significant loss of light transmittance.
BENEFITS OF A RHEXIS-FIXATED EDOF IOL: THE FEMTIS COMFORT
The FEMTIS Comfort IOL (Oculentis) is an asymmetric, refractive, rhexis-fixated extended depth of focus IOL (Figure 1) designed with plate haptics and four additional haptics for capsulorhexis fixation. Made of a foldable hydrophilic acrylic material, called Hydrosmart, the FEMTIS Comfort has an overall length of 10.5 mm and an optic diameter of 5.7 mm. The biconvex optic design includes an anterior near segment (addition 1.50 D) and a posterior aspheric segment.
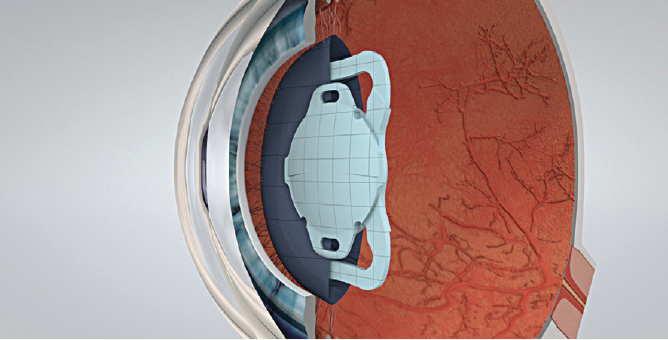
Figure 1. The FEMTIS is designed for rhexis implantation.
The FEMTIS MF15 IOL is currently available in 0.50 D increments from 15.00 to 30.00 D. In the future, the FEMTIS family will expand to include the toric FEMTIS Comfort design.
I recently performed a prospective clinical trial of 50 eyes that underwent laser cataract surgery with the Catalys femtosecond laser (Johnson & Johnson Vision) and implantation of the FEMTIS MF15 IOL to determine the visual results, centration, stability, and overall patient satisfaction.
At 2 months postoperative, 32 eyes were available for follow-up. Of those, 91% were within ±0.50 D of intended refraction, and 97% were within ±1.00 D. With regard to uncorrected intermediate visual acuity at 2 months, 94% were N4 or better at 60 cm and 81% at 40 cm. When I looked at functional vision (combined uncorrected distance and near visual acuities at 40 cm), 100% of eyes were 6/7.5 and N5 or better. Refractive stability up to 12 months is found in Figure 2. There was no incidence of dysphotopsia, IOL decentration, or capsular phimosis.
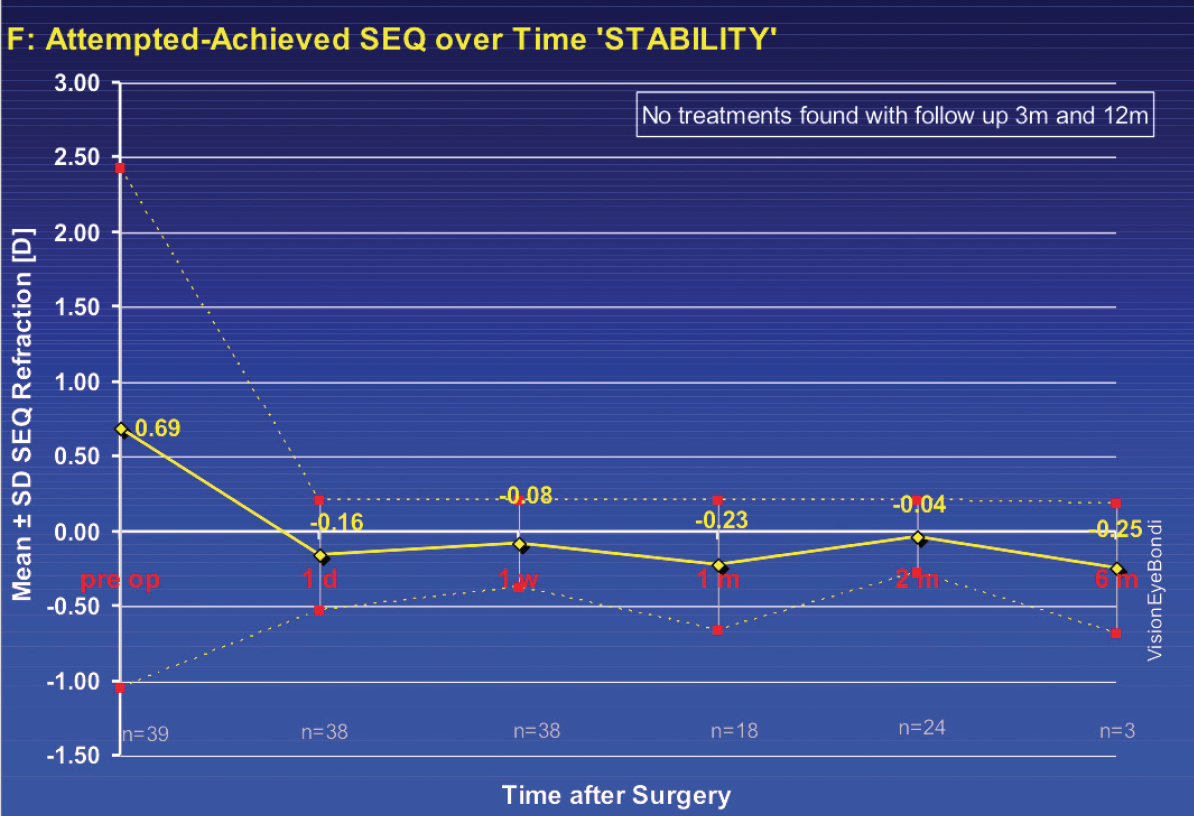
Figure 2. Refractive stability with the FEMTIS IOL.
From these results and from further personal experience, I believe that the FEMTIS Comfort IOL design solves the problems of lens centration, tilt, and rotation as well as provides patients with excellent visual acuity and functional vision.
Lens exchange surgery was uneventful, and on day 1 postoperative the patient observed resolution of his unwanted visual phenomena but did note that his vision remained poor, which was a direct result of the PCO (Figure 3). A Nd:YAG laser capsulotomy was performed 1 month after IOL exchange surgery, and the patient noticed an immediate improvement in his vision (6/6 UCVA, N4 intermediate, and N7 near). He is scheduled to undergo refractive lens exchange surgery in his fellow eye, and we plan to implant the LENTIS MF20 in order to provide the patient with a little extra near vision.
Figure 3. Lens replacement with the LENTIS Comfort IOL, with PCO still present.
CONCLUSION
As demonstrated by this case, patients who are unhappy with their visual results after implantation of a multifocal IOL fare well with a lens exchange procedure. I prefer to use the LENTIS Comfort, as it offers a good functional range of vision and minimizes unwanted visual phenomena. The FEMTIS platform will offer enhanced visual outcomes with the Oculentis EDOF Comfort IOL but may not be suitable for IOL exchange surgery, as it requires a perfect capsulotomy to see its full benefit.
1. Jones JJ, Jones YJ, Jin GJ. Indications and outcomes of intraocular lens exchange during a recent 5-year period. Am J Ophthalmol. 2014;157(1):154-162 e151.
