
Sponsored by STAAR Surgical

Globally, the prevalence of refractive errors is on the rise.1 It should come as no surprise, then, that patients are inquiring about correction of their myopic, hyperopic, and astigmatic errors with greater frequency. Today, therefore, it is almost required that every practice has at least one option for surgical correction to present to patients, whether it be corneal- or lens-based.
Although the safety and efficacy of modern laser vision correction is well documented, there is another option that I prefer for my own refractive cataract surgery practice: the phakic IOL. With near-immediate visual improvement and the removable nature of the procedure, I find that patients are not only drawn to this option initially, but they are also extremely pleased with their results after surgery. By offering the EVO Visian ICL (STAAR Surgical), I can provide my patients with a solution for their refractive errors and select the right patients—with well-judged indications—without the stress of having to recruit enough patients to amortize an expensive excimer or femtosecond laser platform.
KEEP THE PATIENT’S BEST INTEREST IN MIND
Just because I do not offer laser vision correction at my practice does not mean that I steer every refractive surgery candidate toward the EVO Visian ICL. Contrarily, I always have a candid conversation with the patient prior to counseling him or her on surgical options. I ask questions like: “What, in the first place, is pushing you toward seeking refractive correction?” and “What are the biggest barriers in your everyday life that keep you from being happy with your actual vision? For instance, is it spectacles or contact lenses?”
Once I get a sense for the patient and his or her visual needs, I then talk briefly about what options are most appropriate for that individual. Most of the time, at least in my practice, the patient has already read or heard about phakic IOLs and has come in specifically inquiring about this procedure. I then like to challenge the patient on his or her choice of the ICL rather than a laser-based procedure. But if the patient leans toward laser-based surgery and has no contraindications for laser vision correction, I will refer him or her to a competent laser surgeon.
I personally like the EVO Visian ICL because it's a predictable2 procedure, the lens is removable, and the quality of vision it provides patients postoperatively is exceptionally high.3 Other nice things about the EVO Visian ICL are that results are stable4 and, because the optical or mechanical properties of the central cornea are not altered, it does not trigger biomechanical instability the same way that some laser vision correction procedures can.5 Last but not least, implantation of phakic IOLs will not induce or worsen dry eye disease (DED).6 This is extremely important in the region of Switzerland where I live and work—the Valais—because the air is very dry and there is a high incidence of DED in patients who live in my region.
WHY THE ICL?
For a clinic like mine—with a focus on an anterior segment, lens-based surgery—the EVO Visian ICL is a logical addition to the offerings of refractive cataract surgery and refractive lens exchange. The latter procedure can be offered only to a small number of patients who fit very specific criteria, whereas the EVO Visian ICL and its sister lens the EVO+ Visian ICL, with an expanded optic designed for patients with larger pupils, can be safely and more widely indicated. I typically use it in patients between the ages of 25 and 55 years* (Figure 1). A diagram depicting the range of diopters I treat, including the median and mean diopters treated, is seen in Figure 2. Today, it is possible to not only treat high myopia but also low myopia as well with the EVO Visian ICL.
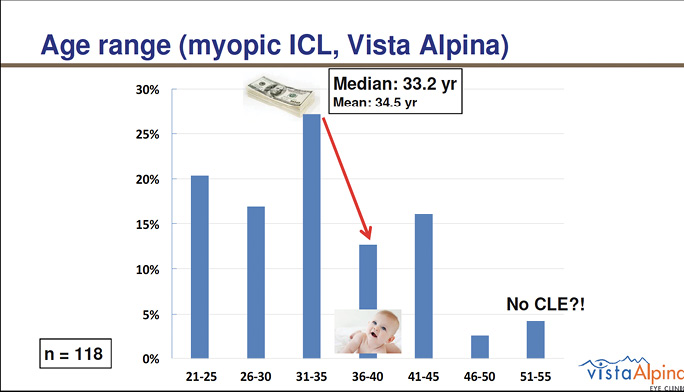
Figure 1. The age range of patients Dr. Vandekerckhove treats with the EVO Visian ICL.
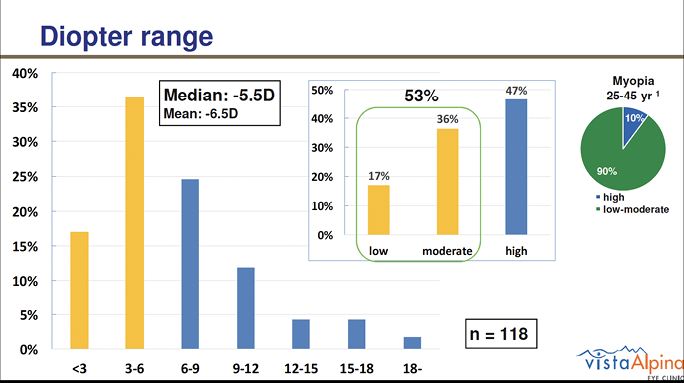
Figure 2. Diagram depicting the range of diopters Dr. Vandekerckhove treats with the EVO Visian ICL, including the median and mean diopters treated.
At my practice, I have been using the EVO Visian ICL for about 4 years now, which was after the KS-Aquaport† was incorporated into the design. The KS-Aquaport, which is essentially a hole located in the center of the optic, helps to optimize the flow of aqueous fluid within the eye. This not only abolishes the need for a preoperative iridotomy, but it has also helped to dramatically decrease the rate of post-ICL cataract as many studies now show.7
In Switzerland, as a country, we may not perform the largest number of phakic IOL implantations in the world, but the number of procedures that I personally perform annually continues to grow. This past year, I implanted about 100 EVO Visian ICLs. I believe that my volume is steadily growing because of the procedure’s predictability and exceptional visual acuity results. In analyzing some of my own recent results (n = 98), the overall refractive predictability of the EVO Visian ICL was 94% within ±0.50 D and 99% within ±1.00 D (Figure 3). Visual acuity results are excellent in the overwhelming majority of cases and tend to be best in patients with low to moderate myopia (Figure 4).
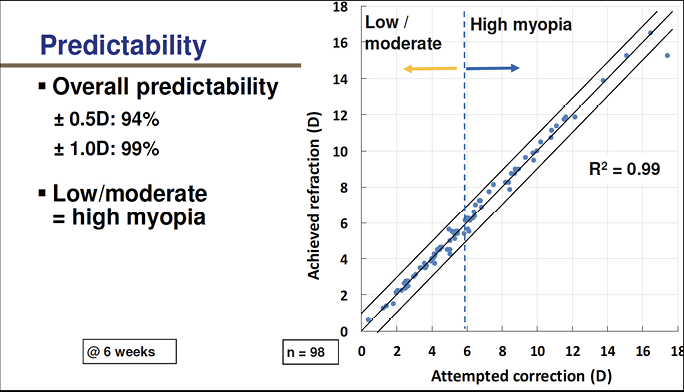
Figure 3. Overall refractive predictability of the EVO Visian ICL in Dr. Vandekerckhove’s practice.
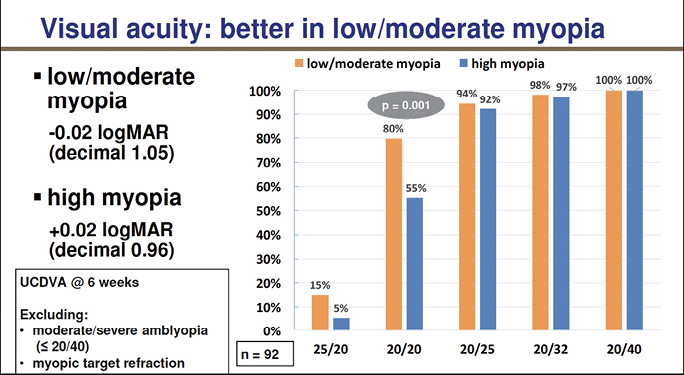
Figure 4. Visual acuity results tend to be best in patients with low to moderate myopia. Six eyes were excluded from the visual analysis because of amblyopic and myopic target refraction.
POSITIONING AND MARKETING
When I first started offering the EVO Visian ICL, I organized quite a lot of patient informational sessions, which I held in the evenings after office hours. But since my volume has grown, I now mainly rely on word-of-mouth to increase my ICL volume further. Today, most people who come in to inquire about the EVO Visian ICL do so because they heard about it from a friend or family member who I previously treated (Figure 5).
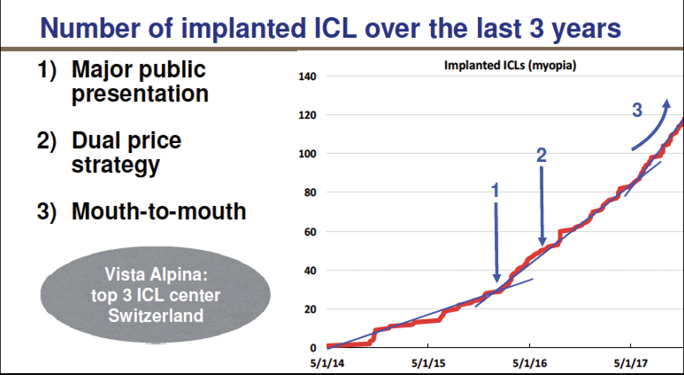
Figure 5. Dr. Vandekerckhove’s marketing strategy for the EVO Visian ICL over the years. Now, most of his patients are referred to him by other patients who have undergone the procedure at his practice.
When patients do present asking for a phakic IOL, I still educate them on all available options, including their benefits and risks. I make sure to mention that all modern refractive correction procedures are very safe and effective. I explain that, with laser, the goal is to modify the optical properties of the cornea in order to induce a refractive change. With the ICL, the goal is to add an optical device—a lens—to induce the refractive change.
The procedures are also completely different in terms of advantages and disadvantages. I position the phakic IOL as a premium option because it is removable; it is more accurate than LASIK,8 especially in the high-diopter range; it is predictable (Figure 6), accurate, and stable in the long term (with virtually no myopic regression, even in the high diopter range); it provides high-quality vision and contrast sensitivity2; and it does not induce DED symptoms.6
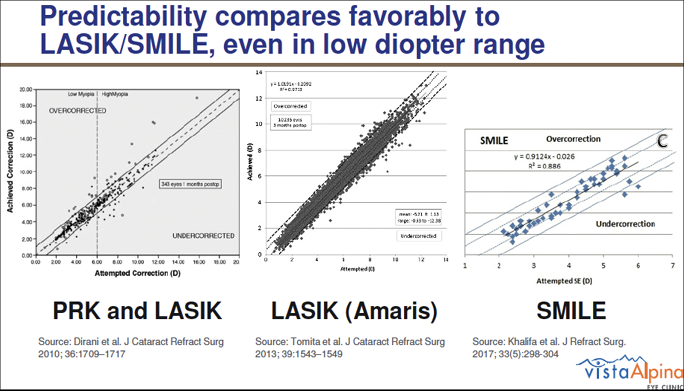
Figure 6. Predictability of EVO Visian ICL implantation versus PRK, LASIK, and small incision lenticule extraction.
For patients who are concerned about the price of the procedure, I emphasize the continued cost of contact lenses and glasses over their lifetime. Deciding to undergoing surgical correction with the EVO Visian ICL is costly; however, in the long run, a couple thousand euros typically should not and does not influence the patient’s decision. I do offer two-tiered pricing, charging 50% more for eyes with higher diopters of correction compared with eyes with low to moderate myopia. I have found that this strategy avoids me charging too much above the price for LASIK in the majority of the patients who I treat (low to moderate myopia).
CONCLUSION
In the end, I believe that, for high-volume anterior segment surgeons, phakic IOLs are a logical option for refractive correction. I have been successfully offering the EVO Visian ICL to my patients for more than 4 years, and despite fierce competition from colleagues who offer laser vision correction procedures, I have found that my surgical volume continues to grow steadily year after year. The key is not to sell the technology (after all, we are doctors) and to center marketing messages around the many advantages of the phakic IOL and less on price.
1. Holden B, Fricke T, Wilson D, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042.
2. Lisa C, Naveiras M, Alfonso-Bartolozzi B, Belda-Salmerón L, Montés-Micó R, Alfonso JF. Posterior chamber collagen copolymer phakic intraocular lens with a central hole to correct myopia: One-year follow-up. J Cataract Refract Surg. 2015;41(6):1153-1159.
3. Sanders D, Vukich JA. Comparison of implantable collamer lens (ICL) and laser-assisted in situ keratomileusis (LASIK) for low myopia. Cornea. 2006; 25(10):1139-1146.
4. Lee J. Long-term clinical results of posterior chamber phakic intraocular lens implantation to correct myopia. J Clin Exp Ophthalmol. 2016;44(6):481-487.
5. Yang E, Roberts CJ, Mehta JS. A review of corneal biomechanics after LASIK and SMILE and the current methods of corneal biomechanical analysis. J Clin Exp Ophthalmol. 2015;6:507. doi:10.4172/2155-9570.1000507
6. Naves JS, Carracedo G, Cacho-Babillo I. Diadenosine nucleotid measurements as dry-eye score in patients after LASIK and ICL surgery. Paper presented at: the American Society of Cataract and Refractive Surgery; 2012.
7. Shimizu K, Kamiya K, Igarashi A, Kobashi H. Long-term comparison of posterior chamber phakic intraocular lens with and without a central hole (hole ICL and conventional ICL) implantation for moderate to high myopia and myopic astigmatism. Medicine. 2016;95(14):e3270.
8. Kamiya K et al. Visual performance after posterior chamber phakic intraocular lens implantation and wavefront-guided laser in situ keratomileusis for low to moderate myopia. Am J Ophthalmol. 2012;153(6):1178-1186.
*In jurisdictions of the EU notified bodies where the CE Mark is recognized, the EVO Visian ICL is indicated for use in myopic patients 21 to 60 years of age.
†The KS-Aquaport was named after and developed in cooperation with Kimiya Shimizu, MD of Japan.
ATTENTION: Please reference the EVO and EVO+ Visian ICL product information for a complete listing of indications, warnings, and precautions.
