




The popularity of toric IOLs has grown rapidly over the past decade. This article details four tips for obtaining the most accurate results when implanting these lenses in patients with corneal astigmatism and sheds light on areas in which further study is warranted.

CONSIDER POSTERIOR CORNEAL ASTIGMATISM
Traditional keratometers, both manual and automated, and corneal topographers measure only the radius of curvature of the anterior corneal surface (in millimeters). They calculate—or, better, estimate—the power of the whole cornea. Because these devices cannot measure the curvature of the posterior corneal surface, they must make assumptions to account for its power and thus obtain the total corneal power and total corneal astigmatism.
AT A GLANCE
- The first step in improving toric IOL outcomes is to rely on total corneal astigmatism rather than keratometric astigmatism.
- It is not accurate to use a single ratio to convert IOL cylinder into corneal cylinder, as some toric IOL power calculators do.
- Future studies to investigate the influence of SIA and the effect of lens tilt on refractive astigmatism after toric IOL implantation are warranted.
The most important of these assumptions is the use of the so-called keratometric index, which is usually equal to 1.3375 and, less commonly, to 1.3315. The keratometric index is a fictitious value that does not correspond to the refractive index of any corneal layer. It is nevertheless used to calculate the power of the whole cornea without knowing the curvature of the posterior corneal surface.
Use of this index leads to some errors. First, the estimated spherical corneal power is higher than the actual total corneal power by about 0.70 D, as measured by ray tracing through both corneal surfaces.1 This error has no effect on the calculation of the spherical power of IOLs for unoperated eyes, as most formulas were developed to be used with corneal power values derived from the keratometric index. However, this error negatively affects the calculation of corneal astigmatism and toric IOLs.
Several studies have shown that posterior corneal astigmatism displays a vertical steep meridian in most eyes.2-5 Unlike the anterior corneal surface, which is in contact with air and has a positive refractive power, the posterior corneal surface is in contact with aqueous and has a negative refractive power. Hence, a vertically aligned steep meridian on the posterior corneal surface generates against-the-rule (ATR) rather than with-the-rule (WTR) astigmatism. The average power of posterior corneal astigmatism is approximately 0.50 D, and this value should be added to anterior ATR astigmatism and subtracted from anterior WTR astigmatism to determine the total corneal astigmatism.
This average 0.50 D value is not fixed but rather proportional to the amount of anterior corneal astigmatism; therefore, a greater posterior contribution can be expected with increasing values of anterior corneal astigmatism.2 Because the corneal astigmatism calculated with the keratometric index (ie, the keratometric astigmatism) neglects information about posterior corneal astigmatism, it tends to overestimate total corneal astigmatism in eyes with WTR astigmatism and underestimate total corneal astigmatism in eyes with ATR astigmatism (Figure 1).2-5
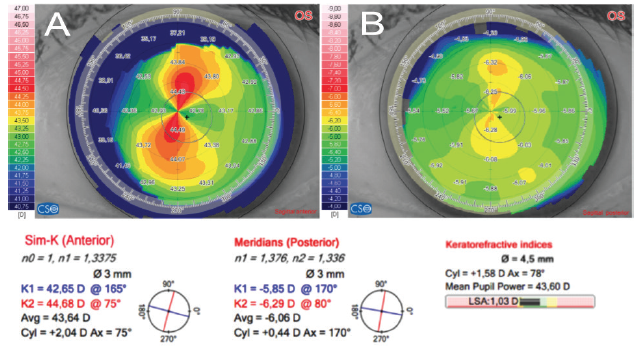
Figure 1. In this eye, the anterior corneal surface shows a vertical steep meridian, leading to an estimation of WTR keratometric astigmatism of 2.04 D @ 75° (A). The posterior corneal surface shows a vertical steep meridian along the same direction, leading to an estimation of ATR astigmatism of 0.44 D @ 170° (B). When posterior astigmatism is taken into account, the calculated total corneal astigmatism is reduced to 1.58 D @ 78°.
We have found that, when calculating cylinder power for toric IOLs, the use of total corneal astigmatism leads to more accurate predictions than keratometric astigmatism, as it reduces astigmatism overcorrection in WTR eyes and astigmatism undercorrection in ATR eyes.6 On the Pentacam (Oculus Optikgeräte), using the value for Total Corneal Refractive Power (ie, the total corneal astigmatism), we were able to reduce residual error in refractive astigmatism after cataract surgery when compared with calculations based on keratometric astigmatism. In eyes with WTR astigmatism, keratometric astigmatism generated an overcorrection of 0.59 ±0.34 D, and this decreased to 0.13 ±0.42 D when total corneal astigmatism was used instead (Figure 2). In eyes with ATR astigmatism, keratometric astigmatism generated an undercorrection of 0.32 ±0.42 D, and this decreased to 0.07 ±0.59 D when total corneal astigmatism was used.
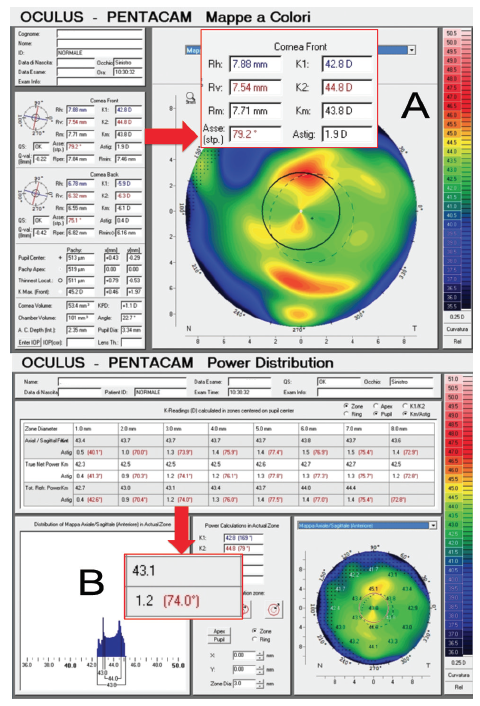
Figure 2. Pentacam measurements in a 71-year-old woman undergoing cataract surgery in her left eye (A). Standard measurements (K1 and K2) show a keratometric astigmatism value of 1.90 D @ 79.2°, which is significantly higher than the Pentacam Total Refractive Power at 3 mm (B), measuring 1.20 D @ 74°.
Minor and clinically insignificant differences were observed in the torsional component of astigmatism, meaning that differences in axis orientation between keratometric astigmatism and total corneal astigmatism are less important than differences in magnitude. Similar results have been confirmed by other investigators.7-9 Therefore, the first step to improve toric IOL outcomes is to rely on total corneal astigmatism rather than keratometric astigmatism.
Something more, however, can be done. In a study that is soon to be published, we observed that the use of total corneal astigmatism is not able to fully eradicate cylinder overcorrection in WTR eyes and undercorrection in ATR eyes.10 Using linear regression to correlate the error in refractive astigmatism to the keratometric astigmatism and total corneal astigmatism as measured preoperatively, we were able to describe equations to optimize these measurements and achieve even better results. With these equations, we were able to raise the percentage of eyes with a refractive error of 0.50 D of astigmatism or less from around 40% to almost 60%.
For this reason, we now rely on what we call optimized keratometric astigmatism to calculate cylinder for toric IOLs and to predict postoperative refractive astigmatism. Similar results can be obtained with the Barrett (unpublished data) and Abulafia-Koch calculators.11 Unfortunately, errors in the prediction of refractive astigmatism will still occur in a considerably large percentage of eyes; this must be taken into account when planning surgical procedures that target plano refraction.

CALCULATE YOUR SIA
Each surgeon should calculate the effect of his or her incision on corneal astigmatism; this value is known as the individual’s surgically induced corneal astigmatism (SIA). Although today cataract surgery through sub–3-mm incisions leads to small variations in corneal astigmatism (usually less than 0.20 D), we suggest calculating the average value for each surgeon. Calculations must be performed through vector analysis. The prediction of SIA, however, can still be inaccurate in some eyes, which can lead to refractive surprises. For this reason, further investigation of SIA is warranted.

DO NOT FORGET ‘CENTRAL’ ASTIGMATISM
Keratometric values generated by optical biometers and simulated keratometry from corneal topographers are usually obtained from corneal curvature readings taken along a ring at a certain diameter from the central cornea. They assume that corneal curvature inside the ring does not change, but that is not always true (Figure 3). In some cases, the typical bowtie is more evident within the ring, and measurements along the ring underestimate the real astigmatism. For this reason, it is wise to look at the map and consider measurements that include the central zone within the ring. This is possible with all devices that use Scheimpflug cameras to measure total corneal astigmatism.
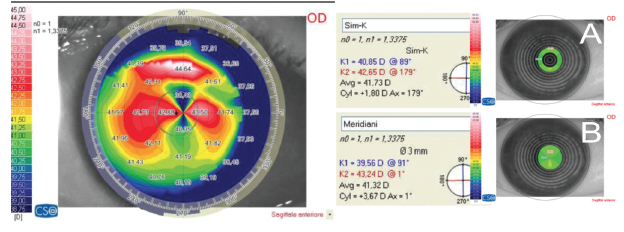
Figure 3. Simulated keratometry (Sirius; CSO), based on the measurements of anterior corneal curvature along a ring, calculates a corneal astigmatism of 1.80 D @ 178° (A). Meridians based on the measurements of anterior corneal curvature inside the ring calculate a higher astigmatism of 3.67 D @ 1° (B).

CONSIDER THE ROLE OF EFFECTIVE LENS POSITION
Toric IOLs are labeled with cylinder power calculated at the IOL plane. This is higher than the cylinder value corrected at the corneal plane. The difference is correlated to the distance between the cornea and the IOL: The higher the distance, the higher the difference.
In other words, in eyes with deep postoperative anterior chambers, such as myopic eyes, a given toric IOL will correct a lower amount of corneal cylinder than in an eye with normal anterior chamber depth, and the ratio between the IOL cylinder and corneal cylinder can be as high as 1.86. In contrast, in eyes with a shallow anterior chamber depth, such as hyperopic eyes, the same IOL will correct a higher amount of corneal cylinder, and the same ratio can be as low as 1.29.12 Therefore, it is not accurate to use a single ratio (eg, 1.46) to convert IOL cylinder into corneal cylinder, as some toric IOL power calculators do.
CONCLUSION
Although our understanding of astigmatism correction has improved considerably over the past decade, refractive surprises can still occur after toric IOL implantation. An error in refractive astigmatism (ie, a difference between the actual and the expected refractive astigmatism) of more than 0.50 D can be found in at least 40% of eyes.
To achieve more accurate results, future research efforts should be focused on multiple issues. First, we hope that better measurements of corneal curvature can be obtained with newer technologies such as OCT, which may be superior to Scheimpflug imaging. Second, the influence of SIA requires further investigation, as previous studies evaluated only anterior corneal curvature changes (with no attention paid to posterior corneal curvature), did not evaluate the influence of measurement repeatability (how much of the observed changes are due to the variability of measurements), and paid little attention to other factors such as the influence of the steep meridian’s orientation. Third and last, no author has yet investigated the effect of lens tilt on refractive astigmatism after toric IOL implantation. These issues will likely all be the subjects of important studies yet to come.
1. Savini G, Hoffer KJ, Schiano Lomoriello D, Ducoli P. Simulated keratometry versus total corneal power by ray-tracing: a comparison in prediction accuracy of intraocular lens power. Cornea [in press].
2. Savini G, Versaci F, Vestri G, Ducoli P, Næser K. Influence of posterior corneal astigmatism on total corneal astigmatism in eyes with moderate to high astigmatism. J Cataract Refract Surg. 2014;40:1645-1653.
3. Koch DD, Ali SF, Weikert MP, et al. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38:2080-2087.
4. Ho JD, Tsai CY, Liou SW. Accuracy of corneal astigmatism estimation by neglecting the posterior corneal surface measurement. Am J Ophthalmol. 2009;147:788-795.
5. Tonn B, Klaproth OK, Kohnen T. Anterior surface-based keratometry compared with Scheimpflug tomography-based total corneal astigmatism. Invest Ophthalmol Vis Sci. 2015;56:291-298.
6. Savini G, Næser K. An analysis of the factors influencing the residual refractive astigmatism after cataract surgery with toric intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56:827-835.
7. Reitblat O, Levy A, Kleinmann G, Abulafia A, Assia EI. Effect of posterior corneal astigmatism on power calculation and alignment of toric intraocular lenses: comparison of methodologies. J Cataract Refract Surg. 2016;42:217-225.
8. Abulafia A, Hill WE, Franchina M, Barrett GD. Comparison of methods to predict residual astigmatism after intraocular lens implantation. J Refract Surg. 2015;31:699-710.
9. Hoffmann PC, Wahl J, Hütz WW, Preussner PR. A ray tracing approach to calculate toric intraocular lenses. J Refract Surg. 2013;29;402-408.
10. Savini G, Næser K, Schiano Lomoriello D, Ducoli P. Optimized keratometry and total corneal astigmatism for toric intraocular lens calculation. J Cataract Refract Surg [in press].
11. Abulafia A, Koch DD, Wang L, et al. New regression formula for toric intraocular lens calculations. J Cataract Refract Surg. 2016;42:663-671.
12. Savini G, Hoffer KJ, Carbonelli M, Ducoli P, Barboni P. Influence of axial length and corneal power on the astigmatic power of toric intraocular lenses. J Cataract Refract Surg. 2013;39:1900-1903.
