

The femtosecond laser has emerged as a revolutionary technology in the field of refractive surgery over the past decade, improving cornea-based procedures such as laser vision correction (eg, flap creation, SMILE) and laser-assisted keratoplasty. More recently, the femtosecond laser has been successfully applied to the crystalline lens to assist in cataract surgery. Presbyopia, which is defined as a gradual loss of accommodation, is believed to be due in large part to an increase in stiffness of the crystalline lens.1 Although different methods have been proposed to overcome the symptoms of presbyopia—such as addition of lenses, monovision, and multifocality—none of these aim to restore true accommodation to presbyopic eyes.
AT A GLANCE
• Although different methods have been proposed to overcome the symptoms of presbyopia—such as addition of lenses, monovision, and multifocality— none of these aim to restore true accommodation to presbyopic eyes.
• With the emergence and success of femtosecond laser technology in ophthalmology, it seemed promising to suggest a noninvasive laser procedure to treat presbyopia by softening the natural presbyopic crystalline lens.
• Ultrashort femtosecond laser pulses can be delivered to and precisely distributed in the crystalline lens in a noninvasive and safe procedure in order to increase lens deformability and, thus, accommodation.
With the emergence and success of femtosecond laser technology in ophthalmology, it seemed promising to suggest a noninvasive laser procedure to treat presbyopia by softening the natural presbyopic crystalline lens. Myers and Krueger first proposed this concept of laser lens modulation for accommodation restoration in 1998.2 If it is possible to reverse the gradual age-related loss of accommodation using an efficient, noninvasive laser procedure, this may become a future mainstay for treating presbyopia.
CONCEPT FOR RESTORING ACCOMMODATION
The concept of restoring accommodation by using an ultrashort-pulsed laser to soften a hard nucleus was introduced in the late 1990s.2 At that time, cutting inside the lens was to be achieved via the effect of photodisruption. The proposed idea was to apply laser pulses to create a shaped intralenticular separation, by both ablating with the laser plasma and cleaving with the expansion of the cavitation bubble. This method would enhance the sliding of the lens fibers and consequently increase the flexibility of the lens, restoring its deformability and accommodative ability.
A crucial point to consider to successfully restore accommodation is the functionality of the other structures involved in the accommodative process in a presbyopic eye. Recent studies have demonstrated the continued contractility of the ciliary muscle and elasticity of the capsule in presbyopic eyes,3,4 allowing the production of the forces required to generate accommodation.
Therefore, given the apparent viability of the accommodative apparatus in the presbyopic eye, photophacomodulation via femtosecond laser lentotomy was proposed as an intralenticular strategy to change the modulus of elasticity of the aging lens.2 This appears to be a promising concept for restoring accommodation.
EXPERIMENTAL STUDIES
The complex microanatomy of the crystalline lens, with its 3-D geometry of overlapping lens fibers and sutures that change with age and lens growth, makes the precise pattern of laser spot placement within the lens difficult to determine and localize. In 2006, Kuszak et al developed a finite element analysis model of the human crystalline lens based on the microanatomy and physiologic function of the lens fibers.5 This model has contributed to the assessment of the impact of specific intralenticular laser microincisions on lens flexibility in order to optimize the sliding and deformation of lens fibers and, hence, to improve accommodation.
After introducing this framework for the development of laser cutting patterns within the lens, several treatment algorithms were tested in a computer-generated model. Patterns evaluated included concentric shells, incisions along lens sutures, concentric cylinders, and a waffle pattern. Treatments both within and sparing the center of the lens were tested; to minimize the potential for visual quality degradation, ablation patterns sparing the center were preferred.5
More recently, an experimental study has been conducted in porcine lenses to evaluate the efficacy of microincisional patterns delivered into the lens to create gliding planes in order to gain deformability.6 These authors reported that a sagittal cutting profile offered better cutting quality and shorter procedure times, and they also showed that the number of sagittal cuts directly correlated with the gain in deformability. The investigators concluded that number, position, and alignment of microincisions in the lens had a proportional effect on deformability and that angulation of the sagittal cutting plane, taking on a conical shape with the cuts extending centrally and posteriorly, could improve the magnitude of deformability.
However, although these findings are useful, because they were observed in experimental in vitro studies they provide only limited information in the quest to determine the most efficacious geometric profile of pulse placement in a living human presbyopic eye, where many other factors have to be considered. The ideal cutting pattern to restore accommodation has not yet been developed, and it will require empirical investigation beyond computer-generated modeling and in vitro laboratory testing. In vivo clinical testing in living patients is required, and these evaluations are now under way.
CATARACTOGENESIS AND SAFETY
To fully provide the benefit of a noninvasive laser procedure to restore accommodation, application of laser pulses inside the lens must avoid inducing opacities. In 2005, Krueger et al conducted the first safety study of femtosecond laser photodisruption in the crystalline lens, aiming to determine the cataractogenic potential of circular and radial cutting patterns in rabbit eyes.7 After 3 months, the treated rabbit lenses showed good transparency relative to their untreated, contralateral controls, and no evidence of progressive cataract formation was seen. Additionally, light scattering was evaluated by performing a scanning laser test of the excised lenses, and no greater scatter was found in comparison with contralateral controls.
Another recent study in rabbit eyes also demonstrated no cataract formation at 6-month follow-up.8 Laser cutting patterns have also been tested in primates prior to proceeding with human clinical studies (unpublished data) because rabbit eyes are considerably different from human eyes. In primate eyes, no progressive cataract formation was observed during 3 years of follow-up. This positive experience finally led to the first clinical series in human eyes, again showing no progressive cataract formation (unpublished data).
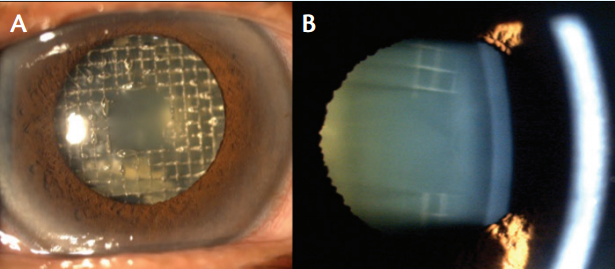
Figure 1. Immediate postoperative aspect of an eye after application of waffle pattern (A). On postoperative day 1, the intralenticular bubbles had faded away, and only pinpoint opacities could be observed in the area of microincisions (B).
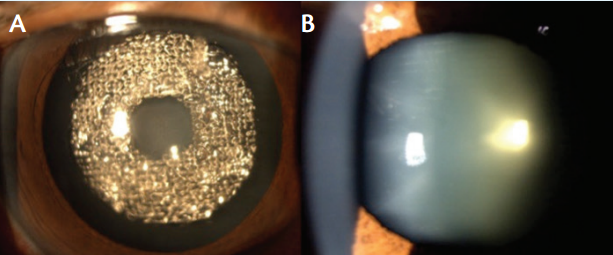
Figure 2. Immediate postoperative aspect of an eye after application of washer pattern (A); crystalline lens on postoperative day 1 (B).
EARLY CLINICAL OUTCOMES
After the earliest clinical attempts in Mexico City by Ramon Naranjo Tackman, MD, as early as 2008, the first series of patients following a clinical protocol was performed by Harvey S. Uy, MD, in the Philippines. Patients between 45 and 60 years old with precataractous lenses (no greater than cataract grade 2) and BCVA of 20/40 or better, who were willing to undergo refractive lens exchange and who could respond both subjectively and objectively to the perceived effects of treatment, were enrolled in this study.
Over the past 2 years, 60 patients have been unilaterally treated, and all participants had the option either to proceed with refractive cataract surgery after 1 month or to delay lens extraction, in which case they would be followed for up to 36 months. The following parameters were analyzed to assess the accommodative and visual effect of the treatment: (1) objective accommodation (Grand Seiko autorefractor), (2) subjective push-down near the point of accommodation, (3) logMAR best distance-corrected near visual acuity, and (4) distance BCVA. Two alternative center-sparing treatment algorithms were used in this study in order to compare their respective efficacy in accommodation restoration: the waffle pattern (Figure 1A) and the washer pattern (Figure 2A).
At 1-month follow-up, 19.2% of patients (n = 10) showed an improvement in objective accommodation with a mean gain of 0.76 ±0.42 D (0.25 –1.50 D), whereas 55.6% (n = 35) showed an improvement in subjective accommodation response to the push-down method with a mean gain of 0.72 ±0.68 D (0.02 – 2.33 D). The mean change in logMAR best distance-corrected near visual acuity (number of logMAR letters change) at 1 month was 7 ±6 letters (range, 1–31), with 40.8% (n = 29) showing an improvement in this parameter.
Regarding safety, no intraoperative complications were reported, including progressive cataract formation. Patients in whom intralenticular bubbles in the visual axis were seen immediately after treatment reported visual disturbances of glare, halos, starburst, and optical distortions. After the first 1 or 2 days, the gas bubbles cleared up, leaving only pinpoint opacities, and patients reported a return to near normal functional vision (Figures 1B and 2B).
Early differentiation in outcomes between the treatment patterns suggests that patterns with lower energy and pulsing might have had a greater effect on restoration of accommodation. Further investigations to determine the most efficacious treatment algorithm are underway to further improve outcomes. Although reliable and significant restorations of accommodation have not been demonstrated yet with the femtosecond laser, the absence of cataract formation and significant symptoms warrants further testing of clinical efficacy with new treatment algorithms. More patients are currently being treated with refined algorithms, and results will be reported as data become available.
CONCLUSION
During the past decade, restoring accommodation in presbyopic eyes moved from a theoretical concept to an experimental reality. Ultrashort femtosecond laser pulses can be delivered to and precisely distributed in the crystalline lens in a noninvasive and safe procedure in order to increase lens deformability and, thus, accommodation.
Technological advances in femtosecond laser refractive and cataract surgery will continue, as will the tremendous interest among patients and physicians in the prospect of restoring accommodation. It is likely that, in the near future, with the optimization of cutting patterns and laser parameters, we will see laser restoration of accommodation becoming a mainstay for treating presbyopia.
1. Glasser A, Campbell MC. Biometric, optical and physical changes in the isolated human crystalline lens with age in relation to presbyopia. Vision Res. 1999;39(11):1991-2015.
2. Myers R, Krueger RR. Novel approaches to correction of presbyopia with laser modification of the crystalline lens. J Refract Surg. 1998;14:136-139.
3. Strenk S, Semmlow J, DeMarco J. Age-related changes in human ciliary muscle and lens: a magnetic resonance imaging study. Invest Ophthalmol Vis Sci. 1999;40:1162-1169.
4. Krag S, Andreassen T. Mechanical properties of the human lens capsule. Prog Retin Eye Res. 2003;22:749-767.
5. Kuszak JR, Mazurkiewicz M, Zoltoski R. Computer modeling of secondary fiber development and growth: I. Nonprimate lenses. Mol Vis. 2006;12:251-270.
6. Ripken T, Oberheide U, Fromm M, et al. fs-Laser induced elasticity changes to improve presbyopic lens accommodation. Graefes Arch Clin Exp Ophthalmol. 2008;246(6):897-906.
7. Krueger RR, Kuszak J, Lubatschowski H, et al. First safety study of femtosecond laser photodisruption in animal lenses: tissue morphology and cataractogenesis. J Cataract Refract Surg. 2005;31(12):2386-23894.
8. Lubatschowski H, Schumacher S, Fromm M, et al. Femtosecond lentotomy: generating gliding planes inside the crystalline lens to regain accommodation ability. J Biophotonics. 2010;3(5-6):265-268.
David Smadja, MD
• Ophthalmology Department, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel
• Researcher Associate at Institute of Nanotechnology and Advanced Materials (BINA), Bar Ilan University, Tel Aviv, Israel
• davidsmadj@hotmail.fr
• Financial disclosure: Consultant (Alcon, Abbott Medical Optics, Ziemer)
