

Ophthalmology is a specialty blessed with a steady stream of innovative new products. Some of this innovation comes from physician-inventors and small startup companies, while other big ideas come from the research labs of major ophthalmic companies. We are fortunate that practicing ophthalmologists can play a role in each of these settings, helping to influence and guide the development of new technologies that can benefit our patients.
Bringing medical devices to market requires huge investments of time and money. The process can take more than a decade and millions of dollars in going from conception to regulatory approval. The more complex the device and the greater its departure from current technology, the more time and money are involved.
AT A GLANCE
• When a new product is brought to market, the more complex the device and the greater its departure from current technology, the more time and money are involved.
• The story of the Tecnis Symfony IOL can be used to illustrate key steps in the process of innovation and the roles that physicians can play in providing input, validating design and clinical performance, and fostering the adoption of new technologies.
• It is important for surgeons involved in the early stages of product development to convey the science and outcomes to their peers as well as to be aware of any potential side effects of a new technology.
The story of the Tecnis Symfony IOL (Abbott Medical Optics) can be used to illustrate key steps in the process of innovation and the roles that physicians can play in providing input, validating the design and clinical performance, and fostering the adoption of new technologies. The Symfony is the first extended range of vision IOL, utilizing diffractive optics to correct presbyopia without the current concept of multifocality. It was developed internally by Abbott Medical Optics, based upon its successful Tecnis one-piece IOL platform.
IDENTIFYING NEED AND SOLUTION
The initial spark for innovation arises from the recognition of a need in the marketplace. Ideas for new products and product refinements usually come from clinicians because we are the ones who see how our patients benefit from current technology and how things could be improved. We see the possibilities, but the challenge for busy clinicians is to share these ideas with industry in thoughtful and constructive ways.
Although there are many presbyopia-correcting IOL options available, particularly in Europe, it is important for clinicians to recognize the continued need for better solutions to the challenging problem of presbyopia. Despite recent advances, the majority of patients undergoing cataract surgery in 2016 still become presbyopic pseudophakes. Loss of accommodation remains a real problem for our patients, and surgeons must continue to work with industry toward innovative solutions.
In the early stages of the Tecnis Symfony IOL’s development, the shortcomings of the available presbyopia-correcting IOLs were well known: night vision symptoms and a near focal point that was too proximal. The Tecnis multifocal low-add IOLs brought improvements on both fronts (Figure 1), but vision in the far-intermediate range was still decreased compared with near vision.
From an optics standpoint, further reducing the add power would begin to compromise the quality of the distance image. A different approach was needed. Nevertheless, recognizing the difficulties and potential pitfalls of developing a technology that was too radically different, the company opted to develop a new application for diffractive optics on its tried-and-true lens platform.
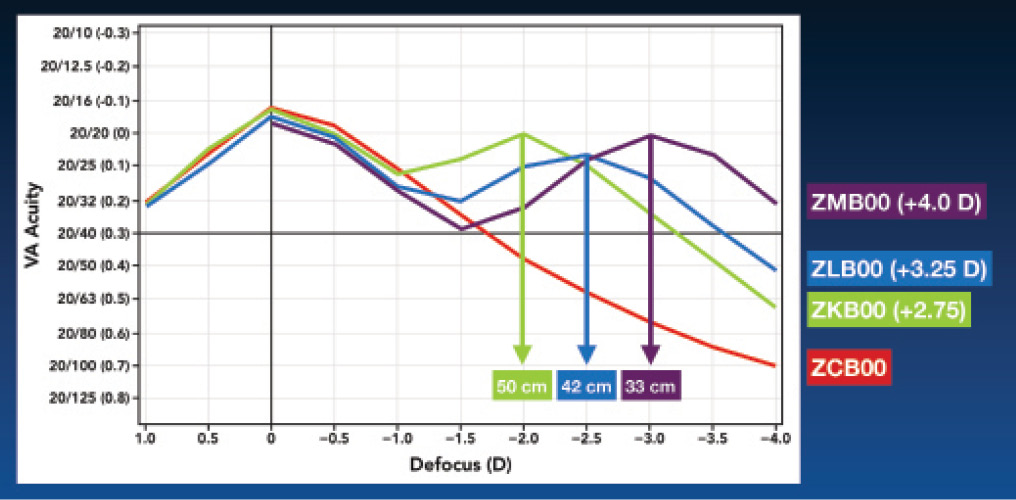
Figure 1. Clinical defocus curves for Tecnis Multifocal IOLs. The location of the peak near focal point is consistent with theoretical laboratory modeling.
NEW DIFFRACTIVE OPTICS
The optic design of the Symfony IOL combines two complementary technologies. First, diffractive achromatic technology, similar to that used in high-end diffractive optics camera lenses, reduces overall chromatic aberration. This helps to enhance contrast sensitivity and, especially when combined with spherical aberration correction, to improve retinal image quality. Second, a proprietary echelette design produces a novel pattern of light diffraction that elongates the focus in the eye. In this way, the lens uses all of the incoming light to produce a continuous range of vision, rather than dividing it into two or three foci (Figure 2).
As a member of the advisory board that first reviewed this lens, I was intrigued by what I learned about the optics. In fact, my initial reaction was that the Symfony is an IOL that I would consider for my own eye—the first time I have felt that way about any presbyopia-correcting technology. It was also appealing to me that only the optics were changed. The lens material, spherical aberration properties, haptic design, implantation technique, and other attributes of the Symfony are identical to those of Tecnis one-piece IOLs.
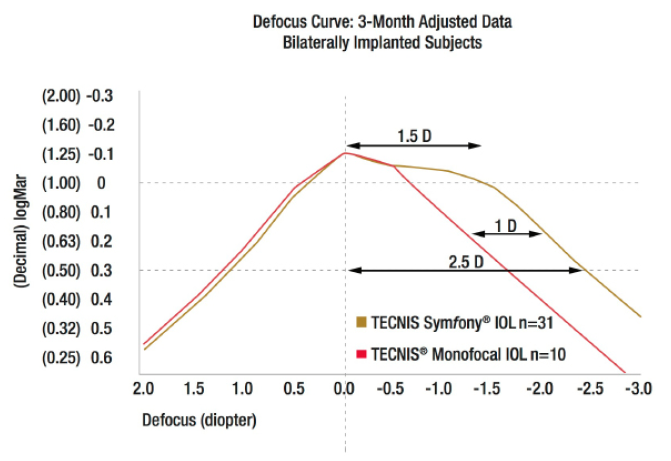
Figure 2. Clinical defocus curve for the Tecnis Symfony extended range of vision IOL. Note the absence of a near focal peak and the broad flat range of vision > 20/20. (Data on file, Abbott Medical Optics.)
BENCH TESTING
Product development is a highly iterative process. In creating the new diffractive optic profile, the optical scientists and engineers at the company produced and tested dozens of designs to find the best balance between quality of vision, range of vision, and the potential for visual side effects.
In order to adequately characterize the optical performance of the Symfony, concurrent advances in the methods of testing IOL optics had to be made as well. The development of these new testing methods may prove to be as important to the continued long-term development of presbyopic IOL technology as the Symfony IOL itself.
With current multifocal and trifocal IOLs, traditional laboratory through-focus curves do not completely characterize their clinical performance. For a monofocal IOL, a target is fixed at optical infinity, and the target spatial frequency is varied to create a modulation transfer function curve for that IOL. For presbyopic IOLs, the target spatial frequency (eg, 50 cycles/mm) is fixed while the target distance is varied (optically with minus lenses) to create a through-focus curve. Two focus peaks are seen for multifocal (bifocal) IOLs, and the peaks on the through-focus curves correlate well with the best focal distances seen clinically. However, the spaces between the peaks on the through-focus curve do not explain why multifocal IOLs clinically produce some (albeit limited) intermediate vision.
Why do traditional modeling methods fall short with presbyopic IOLs, particularly in characterizing intermediate vision? In large part, images in the real world are not composed of a single spatial frequency. Even Snellen letters, which we think of as highly standardized, are composed of multiple spatial frequencies. Therefore, testing a single spatial frequency on a bench is an inadequate way of describing clinical performance.
How then, is it possible to characterize a lens that can provide a continuous range of high-quality vision? During the development of the Symfony IOL, the scientists at Abbott Medical Optics developed a series of innovative bench testing techniques and methodologies that incorporate more data in new ways to achieve a better model of real-world, multispatial vision. Their understanding of these models allowed them to develop the novel optics of the Symfony IOL.
In a European multicenter clinical study,1 more than 90% of patients implanted bilaterally with the Symfony achieved binocular far and intermediate UCVA of 20/25 (0.1 logMAR) or better (mean -0.05 and 0.01 logMAR, respectively), and about 95% were comfortable at intermediate distances without glasses. Moreover, 99% of patients reported no severe night glare or halos. Data from US clinical trials, in which I am an investigator, are not yet available.
PEER EDUCATION
An important role for surgeons who have been involved in the early stages of product development is to convey the new science and outcomes to their peers. The science of chromatic aberration, for example, is a relatively newly understood concept, and it is an important part of what allows the Symfony IOL to provide high-quality vision across an extended range.
Clinical experience can also provide context for study data. Being an investigator provides context for reviewing the clinical trial data. For example, with the Tecnis multifocal low-add IOLs, one might be concerned by the objective rate of halos. But in speaking to patients, many say, “I have halos, but they don’t bother me.” In fact, patient satisfaction with the low-add multifocal IOL was higher than with the monofocal control IOL because patients achieved something they wanted—better functional near and intermediate vision—without being disturbed by night vision problems.
It is also our responsibility as investigators and innovators to be aware of potential visual side effects. Because night vision symptoms are commonly associated with nonaccommodative presbyopic IOLs, understanding and describing those side effects preoperatively helps us to counsel patients who are candidates to receive these IOLs. It also helps us to inform surgeons who may want to incorporate these technologies into their practice. Our goal is to usher in the new technology effectively, so that surgeons can use these products successfully.
CONCLUSION
I look forward to gaining access to the Tecnis Symfony extended range of vision IOL in the United States and to participating in future IOL trials. There are many exciting new lenses and other ophthalmic devices making their way through the research pipeline. It is a privilege to be involved in some small way and to make a meaningful impact on the development and testing of these products.
1. Auffarth G. Clinical Experience with an Extended Range of Vision 1-Piece IOL. Paper presented at: the AECOS European Symposium; June 25-28, 2015; Berlin, Germany.
Daniel H. Chang, MD
• Private practice, Empire Eye and Laser Center, Bakersfield, California
• dchang@empireeyeandlaser.com
• Financial disclosure: Consultant (Abbott Medical Optics, Carl Zeiss Meditec, ClarVista Medical, Omega Ophthalmics)
