



What was once a challenging patient consultation for refractive surgery can now be streamlined. During the past decade, my colleagues’ and my approach to educating patients on their conditions and our understanding of how best to serve their needs has evolved. Years ago, when presbyopic patients would present for LASIK to reduce their dependence on reading glasses and bifocals, we would recommend a refractive lens exchange in cases where there was early lenticular opacity and/or hyperopia. Not infrequently, patients were taken aback at the suggestion of a lens-based procedure. For many years, we performed LASIK in these individuals, and frequently they would come back within 5 to 7 years complaining that their LASIK had “worn off.”
AT A GLANCE
• The term dysfunctional lens syndrome (DLS) characterizes a spectrum of changes that occur with age and that include presbyopia, opacification, loss of image quality, and higher-order aberrations.
• In patients with DLS, it can make more sense to exchange the aging crystalline lens for an appropriately selected IOL instead of performing LASIK now and cataract surgery years later.
Enter the concept of the dysfunctional lens syndrome (DLS) and the use of advanced diagnostics to aid in its detection and proper staging.
what to Know
Below I outline three tips on how to present refractive lens exchange to patients.
Tip No. 1: Use an advanced ocular analysis and include a digital “lens-centric” examination. With this approach, we often find that baby boomers presenting for LASIK do not have clear lenses; instead, they have DLS, a clinical entity that has been overlooked and inadequately characterized for years. The term dysfunctional lens syndrome characterizes a spectrum of changes that occur ubiquitously with age and that include presbyopia, lens opacification, decreased retinal image quality, and higher-order aberrations.1 Part of the rationale behind the terminology DLS is to avoid the use of others such as very early cataract or precataract. These terms can seem dismissive, implying that the patient’s only option is to wait for the early cataract to ripen or for a precataract to become a cataract, delaying surgery by 5 to 10 years.
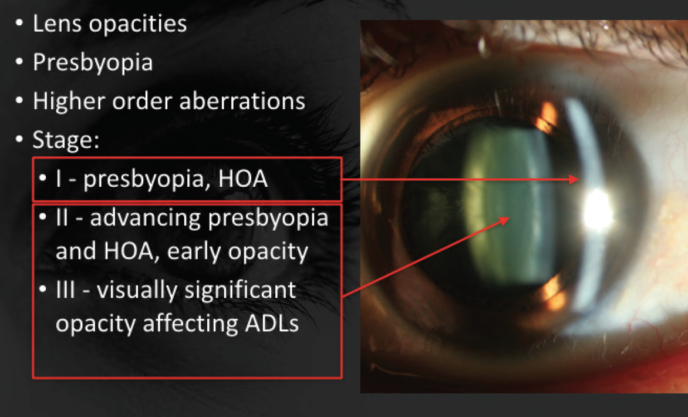
Figure 1. The use of DLS in decision making.
Tip No. 2: Use a DLS grading scale to educate patients on their condition and to suggest the best procedure for them. My colleagues and I recently presented a grading scale for DLS that has been useful in clinical decision-making for a lens- or cornea-based procedure and for educating patients on their condition.2 In stage 1 DLS, the patient has lost the ability to adequately accommodate but still has excellent image quality with a relatively clear lens. In this situation, a cornea-based procedure is often the best choice, unless the patient has a significant degree of hyperopia. In stage 2 DLS, the lens has developed some early opacification, resulting in decreased image quality and higher-order aberrations. In this situation, a lens-based procedure is often the most appropriate choice. In stage 3 DLS, the lens opacities affect the patient’s daily activities and meet subjective and objective insurance-based criteria for a diagnosis of cataract (Figure 1 and DLS by Stage chart above).
As I explain to patients with stage 2 DLS, their situation is similar to looking through two dirty windshields, one in front of the other. We can clean (focus) the outer windshield (the cornea) with LASIK, but the inner windshield (the crystalline lens) is still cloudy. Therefore, in patients with DLS, it makes more sense to exchange the aging crystalline lens for an appropriately selected IOL instead of performing LASIK now and cataract surgery years later. Although we do perform clear lens exchange in younger patients with large degrees of hyperopia, stage 2 dysfunctional lenses are not clear; hence the use of the term dysfunctional lens replacement or refractive lens exchange and not clear lens exchange.
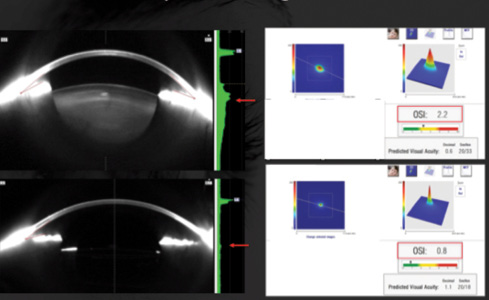
Figure 2. Ocular scatter index (right) before and after refractive lens exchange.
Tip No. 3: Give patients a digital tour of their eyes. Herman Snellen described visual acuity in 1863, but practitioners now have advanced diagnostics that measure functional vision and quality of vision. A patient may have a visual acuity of 20/20 but diminished retinal image quality. Combining the use of dilated Scheimpflug imaging and associated densitometry with double-pass wavefront technology (AcuTarget HD; AcuFocus), we take patients on a digital tour of their eyes, showing them their dysfunctional lens and the correlating light scatter. The AcuTarget HD generates an ocular scatter index, which provides patients with a score for their quality of vision and also demonstrates the light scatter as it falls on the retina (Figure 2).

Ray-tracing technologies like the iTrace (Tracey Technologies) are also being developed to quantify internal aberrations and derive a dysfunctional lens index. I find that showing patients the light scatter (point spread function) and increased ocular scatter index helps them to understand the value of addressing the source of the problem, the aging crystalline lens, with a single procedure, while also preventing the future formation of cataracts.
LISTEN UP
In a discussion with Gary Wörtz, MD, George O. Waring IV, MD, describes his approach to a range of clinical scenarios commonly faced in the management of presbyopia.
CONCLUSION
In our experience, patients who come in for a LASIK consultation and are found to have stage 2 DLS respond well to being told they are candidates for laser vision correction, as we now have lasers to treat both the cornea and the internal lens. Furthermore, during the refractive consultation, we emphasize to all patients that DLS is a normal part of the aging process and that no action is required. For patients with stage 2 DLS who wish to pursue surgery to treat presbyopia, dysfunctional lens replacement/refractive lens exchange is presented as an option. Patients appreciate this as a treatment option, because we educate them appropriately. As with all surgical procedures, we outline the relative risks and benefits of each technique.
1. Waring GO IV. Diagnosis and treatment of dysfunctional lens syndrome. CRST. March 2013;13(3):36-38.
2. Waring GO IV, Rocha KM, Durrie DS, Thompson VM. Use of dysfunctional lens syndrome grading to guide decision making in the surgical correction of presbyopia. Paper presented at: ASCRS/ASOA Symposium & Congress; May 10, 2016; New Orleans, Louisana.
