


Patient satisfaction is a constant pursuit in cataract surgery. In order to enhance the chance of each patient’s postoperative satisfaction, cataract surgeons measure the refraction of the eye preoperatively and attempt to select the appropriate IOL for the patient, based on not only those measurements but also on the patient’s needs and expectations. Many surgeons avoid implanting premium IOLs because of their cost and because of the possibility that the patient will end up unhappy with the visual result.
Regardless of the skill of the surgeon, a multifocal or toric IOL that moves postoperatively will produce an unsatisfactory result and an unhappy patient. And, given current technologies, once an IOL has been implanted, it cannot be adjusted.
Studies suggest that a significant number of patients will require spectacle prescriptions after cataract surgery. For example, a clinical study by Warren E. Hill, MD, found that 37.7% of cataract patients had preoperative astigmatism of more than 1.00 D.1 Pablo Artal, PhD, has reported that postoperative astigmatism of greater than 0.75 D has an adverse effect on the performance of a monofocal IOL.2 Further, about 25.7% of patients who undergo conventional phacoemulsification and about 28% who undergo laser-assisted cataract surgery have a postoperative spherical error of more than 0.50 D, which is enough to adversely affect their distance vision.3
AT A GLANCE
- Preclinical studies with the Perfect Lens refractive index shaping technology have shown that a short (<30 seconds) in-office procedure can adjust acrylic IOL materials such that spherical, toric, and multifocal issues can be resolved permanently.
- The modification of an implanted IOL is achieved by creating a lens within the implanted IOL using the femtosecond laser; the lens created within the implanted IOL is 4.5 mm in diameter and 50 to 100 μm in depth, thus fitting inside the existing IOL optic.
- The Perfector, a mobile machine to house the femtosecond laser, has been designed for use in the office.
Additionally, cataract surgery is generally performed in the elderly population, so most patients who do not choose multifocal IOL implantation will require reading correction postoperatively. Market Scope estimates that more than 90% of postcataract patients are presbyopic. Taken together, all of these factors indicate that more than 50% of patients will require distance correction after cataract surgery, and another 40% will require reading glasses.
Unfortunately, current premium IOLs cannot reliably solve these problems because there is a possibility for the IOL to move postoperatively. Further, the effects of wound healing are unpredictable. Enter the refractive index shaping (RIS) technology in development by Perfect Lens, which can theoretically alter an IOL after it has been implanted and settled in the eye. Preclinical studies have shown that a short (<30 seconds) in-office procedure can adjust acrylic IOL materials such that spherical, toric, and multifocal issues can be resolved permanently. The results are repeatable, and no safety issues have been identified to date. Figure 1 shows an example of the creation of multifocality in a monofocal IOL.
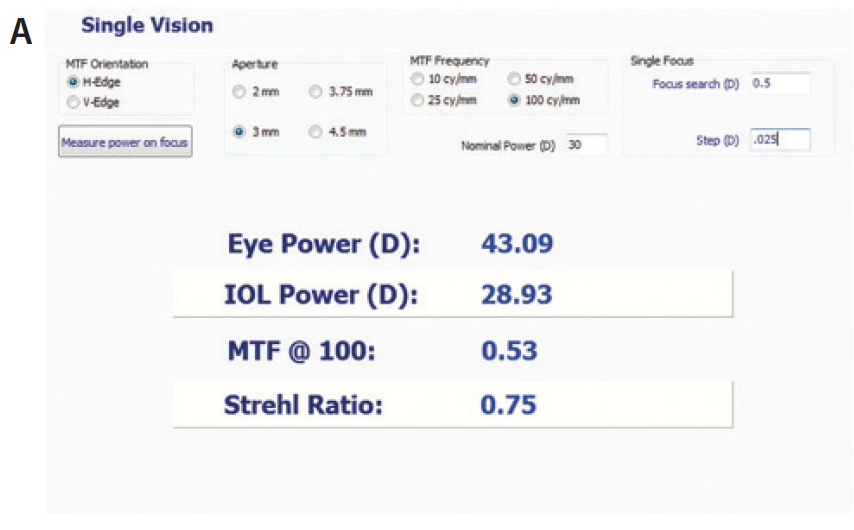
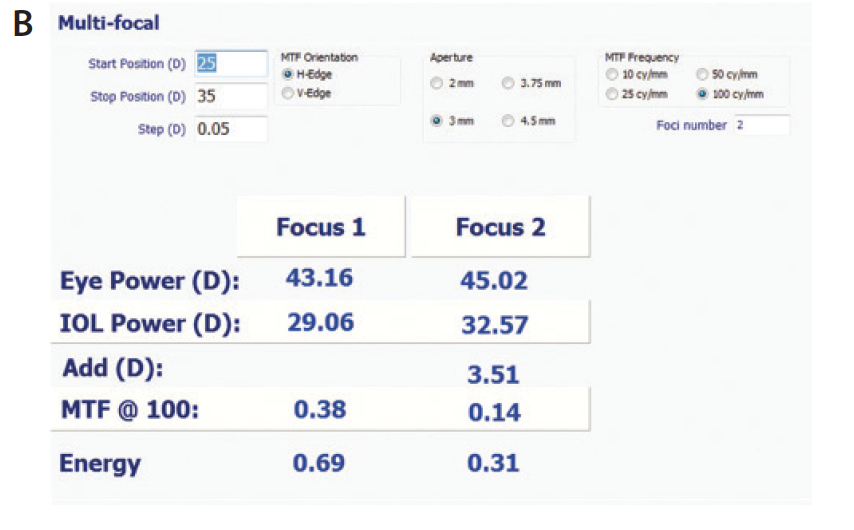
Figure 1. Measurements of an IOL before (A) and after (B) refractive index shape change, showing the creation of multifocality in a monofocal hydrophobic IOL. The targeted change was a 3.60 D add with 70/30 split.
MISSION AND TECHNOLOGY
The RIS technology was conceived in 2009 with the goal of determining a way to modify an acrylic lens, in vitro or in vivo, using a femtosecond laser. The technology alters the refractive index of the acrylic material, and thus alters the refractive characteristics of the IOL.4 This process has been shown to work with a number of standard commercially available hydrophobic and hydrophilic IOLs.5
The modification of an implanted IOL is achieved by creating a lens within the implanted IOL using the femtosecond laser. The lens created within the implanted IOL is 4.5 mm in diameter and 50 to 100 μm in depth, thus fitting inside the existing IOL optic. The lens within the IOL is created by altering the hydrophilicity of the IOL in certain designated areas. This alteration of hydrophilicity causes the subsequent absorption of water by the material, thereby altering the refractive index of the IOL and, thus, its refractive characteristics. The shape, size, and external features of the IOL are unaffected.
PROOF-OF-CONCEPT AND ANIMAL STUDIES
Perfect Lens has conducted a number of preclinical studies with acrylic lenses from five IOL manufacturers (Table 1). In all cases, the RIS technology was able to alter the spherical power by up to 4.00 D, and all changes were within 0.10 D of target. Diminution of modulation transfer function was less than 0.1 lp/mm in almost all situations. No detectable leachables and no significant forward scatter have been seen in studies of these factors to date. The adjustment is stable and should be safe for patients.6
The Perfect Lens RIS system was able to successfully alter the spherical refraction of IOLs implanted in rabbit eyes in tests done at the John A. Moran Eye Center in Salt Lake City, Utah. No inflammation or adverse events were associated with the alteration of the IOL in the rabbit eye, and all modifications were within 0.10 D of target.
USED IN THE CLINIC
A machine to house the femtosecond laser has been designed. The Perfector (Perfect Lens; Figure 2) is mobile, and the machine and procedure are designed for office use. The Perfector uses a proprietary docking attachment that applies less pressure than femtosecond lasers now used in laser-assisted cataract surgery. This low-pressure design will increase patient comfort.

Figure 2. An artist’s conception of the Perfector, designed to be portable for in-office use.
Once the doctor has examined the patient with residual refractive error, the details of the implanted IOL and the desired change to the IOL power are entered into the computer console of the Perfector. The Perfector is attached to the patient with the docking system, and the doctor uses a built-in OCT system to locate the IOL and identify the area within the IOL where the new lens will be constructed. The computer console on the Perfector shows the user exactly where the laser is focused within the IOL. Once the OCT has accurately focused the laser, the doctor initiates the laser. The creation of the lens within the IOL takes less than 30 seconds.
The three most relevant potential uses of the RIS technology in cataract surgery are detailed in the accompanying sidebar.
THREE POTENTIAL USES
1. Removing multifocality from an implanted IOL. For most surgeons, primary barriers to the adoption of multifocal IOLs are the potential risk of postoperative glare and halos and the difficult period for the patient in the postoperative course, during the process of neural adaptation. Unhappy patients require counseling or, in extreme situations, IOL explanation. The Perfector will resolve this issue by offering the doctor the ability to simply remove multifocality from a multifocal lens, thus eliminating the offending halos and glare.
2. Adding premium functions to an implanted IOL. Another aspect of the RIS technology is its potential ability to add premium functions to an implanted IOL. For example, for a patient previously implanted with a monofocal IOL, multifocality could be added if he or she wanted to try life without glasses. Then, of course, if the patient did not enjoy multifocality, the change could be reversed.
3. Adjusting the IOL to fix a change in vision. If the patient’s vision has changed after an IOL was implanted, the surgeon could adjust the IOL to fit the new parameters using the Perfector.
FUTURE OUTLOOK
The ability to alter an implanted IOL would change the way doctors and patients think about IOLs. The permanent nature of cataract surgery would be over, and IOLs would be subject to adjustment as the needs of the patient change.
The Perfector has been shown in vitro to alter the power, asphericity, toricity, and multifocality of hydrophobic and hydrophilic lenses. Perfect Lens plans to begin clinical studies of the RIS technology in the fall of 2017.
1. Holland EJ. Treating astigmatism with torics. CRST. 2010;5-6.
2. Villegas EA, Alcon E, Artal P. Minimum amount of astigmatism that should be corrected. J Cataract Refract Surg. 2014;40:13-19.
3. Manning S, Barry P, Henry Y, et al. Femtosecond laser-assisted cataract surgery versus standard phacoemulsification cataract surgery: Study from the European Registry of Quality Outcomes for Cataract and Refractive Surgery. J Cataract Refract Surg. 2016;42:1779-1790.
4. Sahler R, Bille JF, Enright S, Chhoeung S, Chan K. Creation of a refractive lens within an existing intraocular lens using a femtosecond laser. J Cataract Refract Surg. 2016;42(8):1207-1215.
5. Bille J, Engelhardt J, Volpp HR, et al. Chemical basis for alteration of an intraocular lens using a femtosecond laser. Biomedical Optics Express. 2017;8(3):1390-1404.
6. Sahler R, Bille J, Schanzlin D. In vivo IOL modification. MillennialEYE. 2016;6.
