



Small pupils are a frequent cause for concern among eye surgeons. Because they limit visualization of posterior chamber structures and decrease the working space for surgical maneuvers, small pupils increase the probability of disastrous complications such as iris trauma (iris burn, bleeding, dialysis, or prolapse), anterior and posterior capsular damage, corneal endothelial damage, retained lens material, and suboptimal IOL positioning (out-of-the-bag placement, toric IOL misalignment).
AT A GLANCE
- Screening the eye for pupil problems starts with taking a careful medical and ocular history.
- Following a small-pupil management algorithm can guide the surgeon to methodically achieve adequate pupil size while minimizing risks.
- A range of pharmacologic agents and mechanical expansion devices allow each eye to be matched to the appropriate solution for optimal surgical visualization.
Less serious but potentially troublesome postoperative sequelae of surgery through a small pupil include increased postoperative inflammation, postoperative visual disturbances due to iris defects, suboptimal visual outcomes due to eccentric pupils, and glaucoma due to anterior iris prolapse.
This article details five fundamental facts for conquering the small pupil in cataract surgery.

AN OUNCE OF PREVENTION IS WORTH A POUND OF CURE
There is no standard size that defines a small pupil. In my practice, I employ corrective measures when the maximal pharmacologic pupillary dilation is less than my default capsulorrhexis size of 5 mm. An ounce of prevention is worth a pound of cure, so careful preoperative evaluation of each eye for potential pupil issues helps identify the likely troublemakers.
Screening the eye for pupil problems starts with taking a careful medical and ocular history. Does the patient have a history of neurologic or prostate problems with intake of alpha-blocker medication? What about a history of uveitis, topical corticosteroid use, topical pilocarpine use, glaucoma, or ocular trauma? Dilated slit-lamp examination provides a representative picture of the surgical field and allows the surgeon to devise an appropriate surgical plan.

FOLLOWING AN ALGORITHM CAN BE HELPFUL
At Peregrine Eye and Laser Institute, we developed a small-pupil management algorithm to guide us in systematically addressing suboptimal pupils (Figure 1). The first step is to use topical and intracameral pharmacologic agents and viscodilation. If this is unsuccessful, a careful examination of the semidilated pupil may disclose pupillary adhesions or membranes that may be freed or removed using surgical instruments such as a the Beehler pupil dilator, Graether collar button, or Kuglen hook. A second attempt at pharmacologic dilation may be made after synechiolysis or membrane removal. The ultimate resort is to apply self-retaining pupil-expansion devices, which are generally successful at attaining sufficient pupil size and supporting iris tissue. Surgery may then proceed safely with improved iris stabilization and lens visualization.
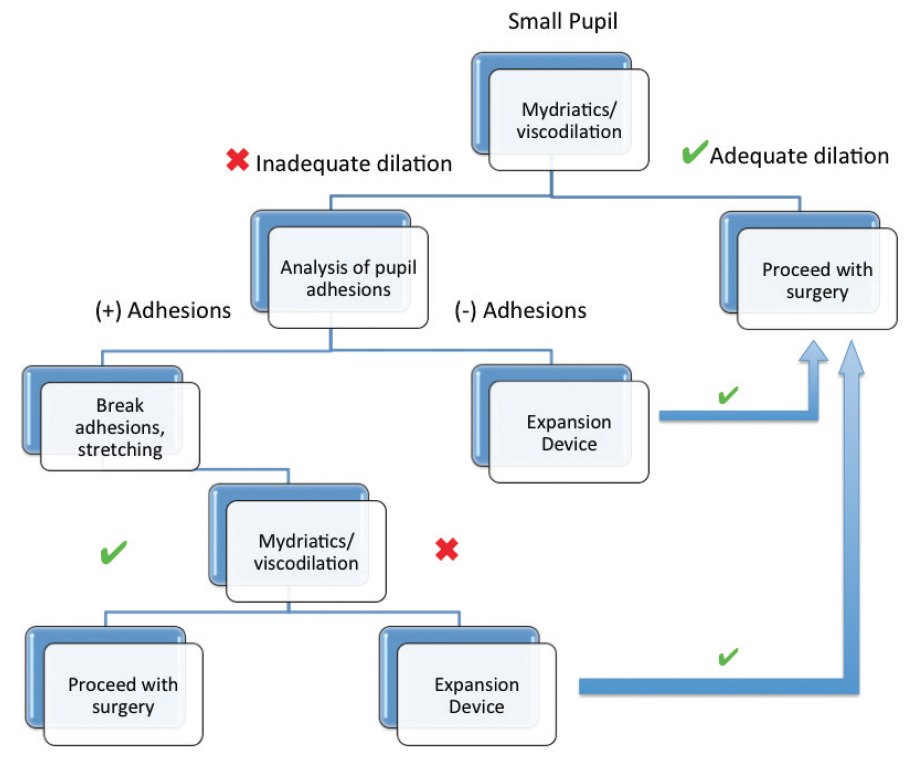
Figure 1. The algorithm used at the Peregrine Eye and Laser Institute for management of small pupils.

PHARMACOLOGIC DILATION IS STANDARD PRACTICE
Use of pharmacologic agents is standard practice for pupil enlargement. The first step for managing small pupils is achieving maximum possible pharmacologic dilation using various formulations. These include topical mydriatics (phenylephrine 2.5% or 10%), topical cycloplegics (tropicamide 1%), and topical nonsteroidal antiinflammatory agents. Intracameral epinephrine HCl 0.01% and lidocaine can also be instilled in combination, providing both mydriatic stimulation and anesthesia should additional maneuvers be required.
Viscodilation using an OVD is often successful in obtaining adequate pupil size for surgical visualization. A recently introduced irrigation fluid additive consisting of phenylephrine 1% and ketorolac 3% (Omidria; Omeros) has been reported to be useful in preventing intraoperative miosis and postoperative pain.

WITH INADEQUATE PHARMACOLOGIC DILATION, CHECK FOR ADHESIONS
If pharmacologic dilation is inadequate, careful inspection for pupillary adhesions should be performed. Incomplete pharmacologic dilation may reveal synechiae or pupillary membranes that can be lysed via membranectomy or removed with fine forceps. Excessive mechanical stretching may cause sphincter tears, which can result in irregular or enlarged pupils. Although synechiolysis and/or pupillary membrane peeling may be indicated, mechanical stretching should be performed with extreme caution to avoid iris damage.
Mechanical stretching of the pupil sphincter may be performed under OVD with an instrument such as a Kuglen hook, collar button, or retractor. Repeated application of intracameral epinephrine and viscodilation can then be reattempted. Even when mechanical stretching does not lead to desired dilation, the incremental pupil dilation may facilitate subsequent insertion of pupil-expansion devices.

A NUMBER OF TOOLS FOR MECHANICAL EXPANSION ARE AVAILABLE
When inadequate dilation still persists after pharmacologic attempts and stretching maneuvers, or when the pupil is floppy, unstable, or eccentric, we resort to the application of self-retaining pupil-expansion devices in order to (1) maximize pupil dilation, (2) stabilize the pupil sphincter, (3) center the eccentric pupil, and (4) protect the iris from surgical trauma.
An ever-growing selection of pupil-expansion devices is available to ophthalmic surgeons. Table 1 provides a partial listing of some commercially available models, and Figure 2 shows several options in clinical use. Due to space constraints, I will discuss only those that we regularly use in our practice.
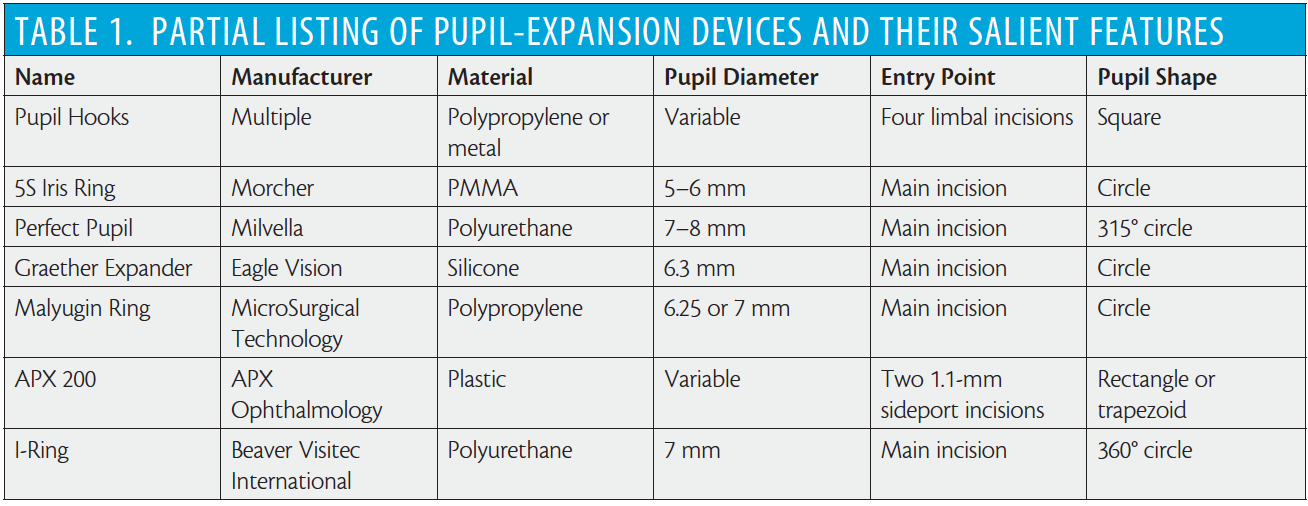
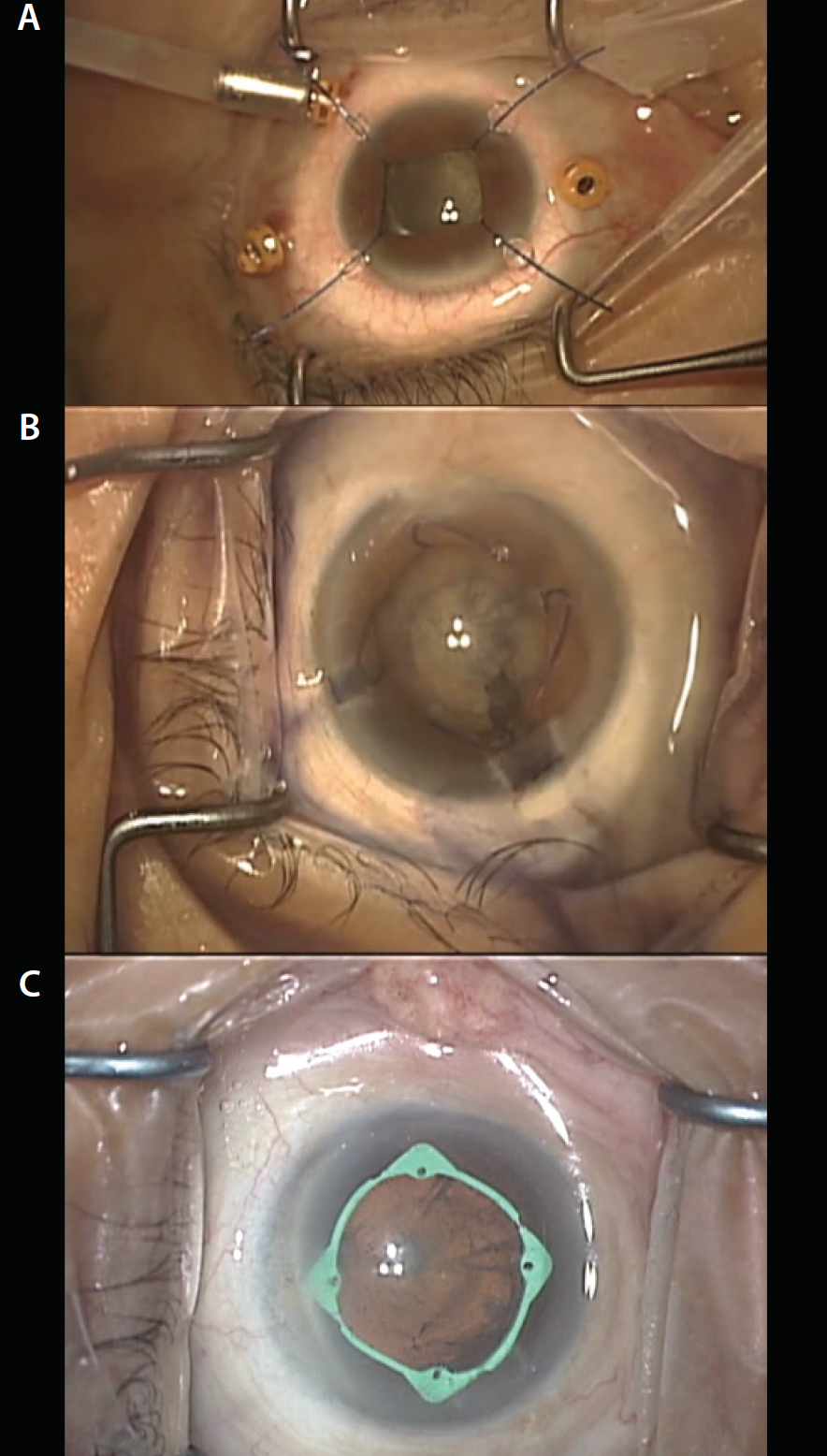
Figure 2. Surgical microscope view of pupil-expansion devices: pupil hooks (A), Malyugin Ring (B), and I-Ring (C).
Pupil hooks. Pupil hooks come in a variety of materials (metal, plastic) and designs. Their main advantage is that they can also simultaneously be used to support the capsular bag in the presence of zonular weakness. The application of pupil hooks is tedious because an additional limbal incision is needed to anchor each hook. Typically, four hooks are applied to achieve a large, square pupil. Another drawback is the tendency to focus stretching forces on a few points on the pupil sphincter, which causes overstretching and can result in iris trauma intraoperatively or irregularly sized pupils postoperatively. Removal of pupil hooks is also time-consuming, as each hook must be separated from the pupil edge and removed through its limbal incision.
Pupil expanders. The Assia Pupil Expander (APX 200) features two scissor-like, spring-loaded devices. One unit is anchored at the limbus and allows the internal arms to swing back and dilate the proximal half of the pupil. A second unit is placed on the opposite side of the cornea to dilate the other half of the pupil and produce a rectangular or trapezoidal shape.
Self-retaining rings. Self-retaining pupil rings are designed to gently distribute stretching forces over the entire pupil margin and thus minimize iris trauma. Many rings, including the 5S iris ring (Morcher), Perfect Pupil (Milvella), Graether expander (Eagle Vision), Malyugin Ring (MicroSurgical Technology), and Visitec I-Ring Pupil Expander (Beaver-Visitec International), come with dedicated inserters, which facilitate insertion into the anterior chamber through the main surgical incision. Once in the anterior chamber, the rings can be guided into position using simple hooks passed through sideport incisions.
With the Malyugin Ring and the I-Ring, removal of these devices at the end of surgery is facilitated immensely by use of the same devices used for insertion. These devices have built-in prongs that engage the ring and pull it out of the eye.
We have used all of the aforementioned devices, but we have the most experience, more than 40 cases, with the I-Ring. This single-use device comes in a preloaded case. The only preparation needed is to completely draw back the plunger of the inserter, which causes the prongs to draw the I-Ring into the inserter. The inserter is then ready for use.
The I-Ring is easily injected through a 2.2-mm incision into the anterior chamber. A Sinskey hook is used to engage the hole of the distal channel and guide the distal channel to capture the pupil edge. The same maneuver is then repeated to engage the pupil edges into the proximal and then lateral channels. This results in a remarkably circular pupil, 6.3 mm in diameter, which provides more than adequate visualization of posterior chamber structures. No additional incisions are created. Deployment of the I-Ring is usually completed in less than 1 minute.
The I-Ring demonstrates outstanding horizontal and vertical stability because the channels securely engage the pupil edges. We have used this device for secondary IOL implantation and vitrectomy surgery in aphakic eyes without capsular elements. The I-Ring stayed in place despite extensive surgical maneuvers in these eyes.
The channels also protect the pupil edges from unintentional damage due to contact with surgical instrumentation. This may lessen postoperative inflammation. Removal of both the Malyugin Ring and I-Ring at the end of surgery is immensely facilitated by using the same insertion devices, which have built-in prongs, to engage the rings and draw them back into the inserter for safe removal. The I-Ring is easily removed by deploying the prong, engaging the proximal or distal hinges, and drawing the plunger back, causing the device to gently return into the insertor cartridge. In cases in which there is significant wound edema that compromises visualization of the proximal ring, or when the main surgical incision is placed too anteriorly, making it awkward to engage the proximal device edge, the soft I-Ring can be engaged on the distal hinge and safely withdrawn using a reverse flip technique.
CONCLUSION
Multiple technological advances over a span of many years have made it possible for the modern cataract surgeon to overcome the challenges of small-pupil surgery. Following a small-pupil management algorithm can guide the surgeon to methodically achieve adequate pupil size while minimizing risks. A wide range of pharmacologic agents and mechanical expansion devices now allow the surgeon to match each eye to the appropriate solution in order to achieve optimal surgical visualization.
Suggested Reading:
Agarwal A, Malyugin B, Kumar DA, Jacob S, Agarwal A, Laks L. Modified Malyugin ring iris expansion technique in small-pupil cataract surgery with posterior capsule defect. J Cataract Refract Surg. 2008;34(5):724-726.
Graether JM. Graether pupil expander for managing the small pupil during surgery. J Cataract Refract Surg. 1996;22(5):530-535.
Grob SR, Gonzalez-Gonzales LA, Daly MK. Management of mydriasis and pain in cataract and intraocular lens surgery: review of current medications and future directions. Clin Ophthalmol. 2014;8:1281-1289.
Osher RH, Ahmed IK, Demopulos GA. OMS302 (phenylephrine and ketorolac injection) 1%/0.3% to maintain intraoperative pupil size and to prevent postoperative ocular pain in cataract surgery with intraocular lens replacement. Expert Rev Ophthalmol. 2015:10;2;91-103.
