



A responsible business model for laser cataract surgery must take into account the increased costs associated with use of the femtosecond laser, along with the more traditional elements such as materials, marketing, surgeon time, and OR or ambulatory surgery center (ASC) space. Although surgeons across the world have documented success with laser cataract surgery, it remains to be seen whether femtosecond laser technology is really the future of the surgery. Currently, the added technology is not reimbursed by US Medicare and other insurance carriers as a separate line item, so it is up to ophthalmologists to decide when it should be offered and under what circumstances, in accordance with applicable US Centers for Medicare and Medicaid Services (CMS) guidelines.
Doing laser cataract surgery increases operating time and cost, but this can be generally outweighed by the possibility of better outcomes. The technology can perform precise placement of arcuate incisions and capsulotomies, and it can achieve lens defragmentation that in our experience reduces phacoemulsification time and energy, potentially leading to clearer corneas in the early postoperative period. The possibility for better outcomes equates to happy patients, which in turn can create practice-wide confidence in the technology and result in more conversions and potentially even more patient referrals.
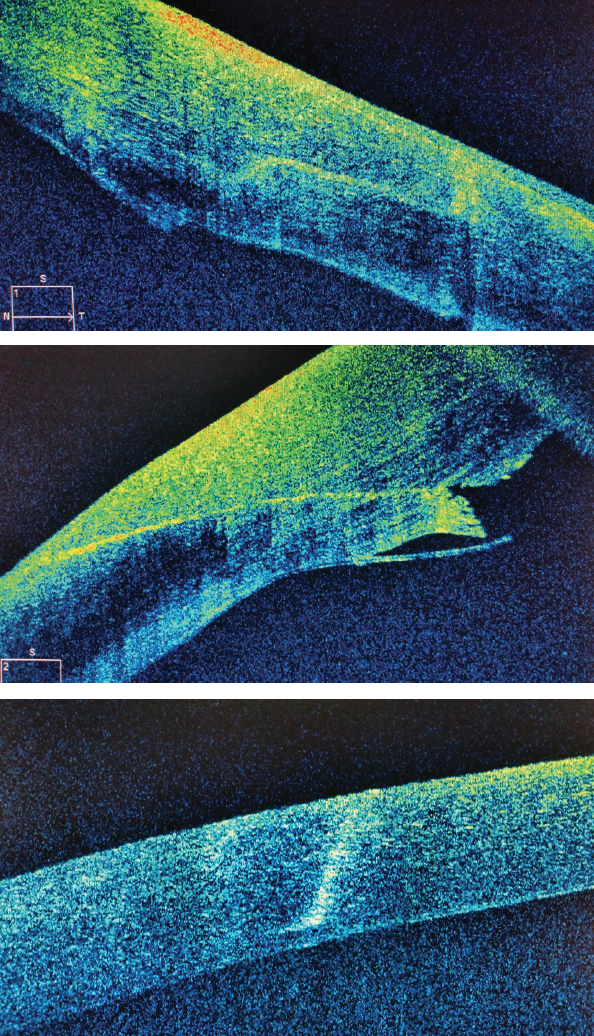
Figure 1. OCT of a laser cataract incision showing tight wound closure and precise interlocking architecture (top), and an OCT of manual keratome incision for comparison (middle). OCT of arcuate incision made with femtosecond laser demonstrating 90% corneal depth (bottom).
EDUCATING PATIENTS
Now more than ever, cataract surgery can offer individuals an opportunity to dramatically improve their vision, with positive impacts on their lifestyle and independence. This is in part due to technology advancements, including comprehensive guidance systems and laser features dedicated to helping surgeons manage astigmatism.
Because patients are essentially deciding what type of vision they want when choosing a procedure, educating them about various options available is essential. However, it is important that this process does not oversell the procedure or its outcomes, and it must remain realistic, customizable, and effective for each individual patient and his or her needs. For pointers on how to educate patients on laser cataract surgery, see the accompanying sidebar below.
POINTERS FOR TALKING TO PATIENTS
I describe laser cataract surgery to my patients by using pictures (Figures 1–4) and video for visualization and analogies that make it easier to understand the concepts. Many patients have the misconception that cataract surgery is and has always been done by laser. Therefore, it is important to start off by educating them about the differences between the laser and ultrasound, how each one works, and which stages of cataract surgery they are used in.
I describe the difference between using a manual keratome or blade versus the laser to create an incision in terms of location, precision, and wound architecture. Visuals, including anterior segment OCT of the cornea and slit-lamp images, help compare and contrast the differences (Figure 1). I often ask patients which images they think were created by the laser, and they are almost always correct. When they look at the precision of the dice patterns (Figure 2) and two-plane chop (Figure 3), they are always fascinated.
Analogies make it easier and faster for patients to understand new technologies. For laser fragmentation, I describe the process as either taking ice cream and putting it in the microwave for a few seconds or dipping Oreos in milk to soften them. When we do fragmentation, I tell them, the nucleus can be aspirated much more quickly and effortlessly in the second, nonlaser part of the surgery.
I always explain to patients that use of the laser will mean that their procedure will take more time, although sometimes we are talking only about seconds. I tell them that they will feel some cold water and pressure when the device is docked (Figure 4). I also alert them to understand why they will not receive sedation during this part of the procedure. Additionally, I warn patients that not everyone is a good candidate for laser cataract surgery. Posture, facial anatomy, and anxiety can sometimes mean we cannot complete the laser procedure, but we may not know this until we attempt it. Still, it is worth a shot. It is always worth a shot.
how to charge
In the United States, charging a premium for laser cataract surgery can be done responsibly when guided by CMS policy. In other parts of the world, including Europe, surgeons can use comparable guidelines to responsibly charge the premium for laser cataract surgery. This includes using the laser, in conjunction with premium IOLs, to perform refractive arcutate incisions to manage astigmatism and to provide better outcomes based on documented surgeon data.
Based on CMS guidance, it is easier to include laser cataract surgery with a refractive package that may also include premium IOLs or astigmatic correction. For toric or multifocal IOL patients, we always use the femtosecond laser because we have doucmented and believe that it helps us achieve the most accurate outcomes.
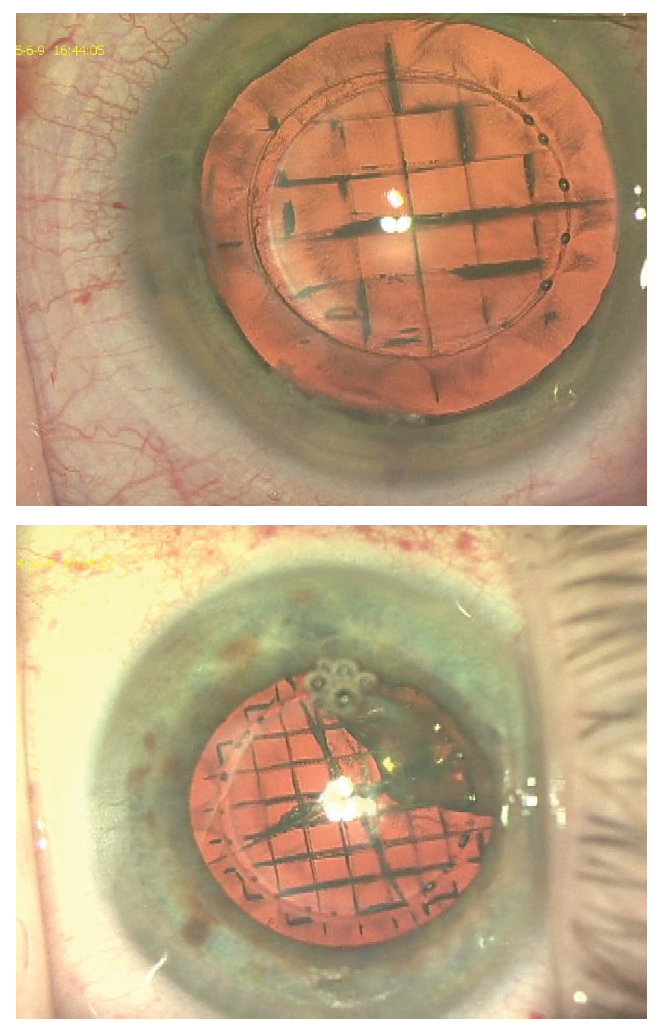
Figure 2. Intraoperative laser cataract surgery image showing defragmentation and quadrant creation (top). It is helpful to show images like these to patients to explain the laser’s role. Another example of the femtosecond laser performing fragmentation of the nucleus (bottom).
breakdown of costs
Charging responsibly also means providing to patients a clear breakdown of the costs associated with using the laser and a clear explanation of the risks, benefits, and alternatives to treatment, including a personalized comparison to traditional cataract surgery. It requires not only that the surgeon believe in the advantages and benefits of the femtosecond technology, but also that the staff is on board and on the same team. Physicians doing laser cataract surgery must truly believe in it.
We discuss with patients why laser cataract surgery is not covered by insurance. I explain that it can be considered a method to upgrade their surgery compared to a traditional procedure, but I emphasize that it is optional. I make it clear that it is their choice and preference whether and how they want their surgery to be customized. In every case, I ensure that patients who elect to have a laser procedure sign an Advance Beneficiary Notice.
I often tell patients that they can achieve a good outcome regardless of whether they choose to opt for laser cataract surgery; however, I say, the laser offers unique advantages. These include the ability to address astigmatism at the time of surgery with exemplary precision and to achieve increased precision with less ultrasonic energy applied to the eye. I explain to them why I like using the laser and that I believe its benefits are worth the additional costs. I tell them that our laser can scan the lens and customize the treatment accordingly, and it can communicate wirelessly with our preoperative testing to reduce errors. I also explain to patients why we invested in the laser several years ago and how it has positively changed the landscape of cataract surgery.

Figure 3. Laser capsulotomy and two-plane chop facilitate easy nucleus disassembly.
Finally, it is important to make it clear to patients that the laser itself does not drive the success of the entire procedure. That depends rather on the surgeon’s skill and what outcomes the surgeon has demonstrated with the laser in his or her hands.
For an overview of the CMS guidelines that surgeons in the United States must follow, including the importance of documenting the use of femtosecond technology in your hands, see Understanding the CMS Guidance below.
Understanding The cms GUIDANCE
In the United States, the CMS is very specific about when surgeons can and cannot charge for the use of a femtosecond laser during cataract surgery. Below are a few tips based on my interpretation of the guidelines. Surgeons are encouraged to review the guidelines put forth by the CMS, which are available on www.cms.gov, and to check their local governing bodies for further guidance.
If a femtosecond laser is used during cataract surgery in which a premium IOL is implanted, surgeons may charge extra for the difference in fees between standard and premium IOLs and for the time and effort of performing any additional testing, imaging, or procedures prior to the surgery, assuming these are not already routinely done as part of the standard cataract procedure.
A refractive procedure performed at the time of cataract surgery can be billed to the patient. This includes arcuate incisions created by a femtosecond laser as a means to correct astigmatism.
A surgeon is allowed to charge a patient for the use of a femtosecond laser if:
1. The surgeon has clinically demonstrated and documented that performing this type of procedure could benefit the patient and/or increase the likelihood of achieving the patient’s desired outcome; and
2. The patient has provided consent. The signed patient consent form should serve as evidence of the treatment discussion and agreement by the patient regarding his or her responsibility for payment of noncovered services to achieve the desired outcome. The surgeon’s clinical recommendation should be recorded in the patient’s chart.
OTHER COSTS
Business planning for laser cataract surgery must take into account the amount and cost of training staff members on the use of the laser. Marketing costs to promote the laser, so that it doesn’t turn into a US$500,000 paperweight, must be considered. For some practices, the laser can complement a variety of existing refractive packages.
Lasers with a large footprint can take up valuable space in the OR or ASC, and this must be taken into consideration for patient flow and scheduling. However, there are lasers with smaller footprints that have taken this into consideration. Maintenance costs and service contracts can add up, and per-click fees can grow over time. All of these factors must be considered in the business forecast.
Moreover, preparations must be made regarding what to do if a patient has paid for laser cataract surgery but the procedure cannot be completed or must be aborted. We emphasize to patients that the cost for a premium IOL is the same with or without the laser. This helps to streamline cost and lens options for patients, and I find this also takes away the purchasing barrier and enables me to use what I believe is the best technology for the patient.
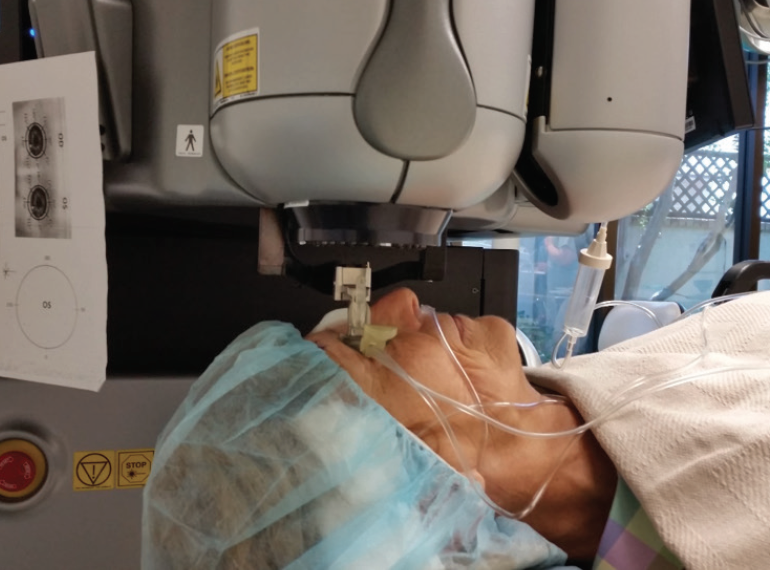


Figure 4. Patient docked to femtosecond laser (top); review of scans, patient anatomy, and treatment plan prior to engaging laser treatment (center); the old method of manually marking the patient in an upright position prior to toric lens implantation (bottom).
CAN WE AFFORD NOT TO?
The most important business question for practices in competitive, saturated markets is not “Can we afford to offer laser cataract surgery?” but rather “Can we afford not to?” Today’s cataract patients have high expectations of their vision after cataract surgery, and it can only be imagined that the expectations of patients in the future will continue to rise. The femtosecond laser may be the answer to meeting those growing expectations.
Practice owners must ask themselves whether they truly believe in the difference offered by laser cataract surgery and whether that difference is important enough to try to overcome decreases in efficiency and increases in cost. This is the elephant in the room with the laser, and it must be addressed if a facility is willing to take on the challenges of laser cataract surgery and chart a clear path toward better surgical results.
1. Gavris, M, Horge I, Avram E, Belicioiu R, Olteanu IA, Kedves H. Fuchs endothelial corneal dystrophy: Is femtosecond laser-assisted cataract surgery the right approach? Rom J Ophthalmol. 2015;59(3):159-163.
2. Roach L. Challenging eyes do well with laser cataract surgery. https://www.medscape.com/viewarticle/804933. Accessed January 23, 3018.
