




A look back at the 2007 article by Georges Baikoff, MD, excerpted below, shows that the history of phakic IOLs is long and complex, reaching back to the 1950s. Many styles have come and gone since that time. His article is full of company and phakic IOL brand names that few young surgeons may remember today: The Phakic Refractive Lens (PRL, Ciba Vision), the Adatomed Implant (Chiron Adatomed), the Vivarte (IOLTech), and even Professor Baikoff’s own ZB5M (Domilens) are long departed from the market.
An excerpt from CRST Europe September 2007
Refractive Phakic IOLs of Then and Now
Herein, I share the development of and experience with these implants.
By Georges Baikoff, MD
In the 1950s, José Ignacio Barraquer, MD, of Spain; Benedetto Strampelli, MD, of Italy; M. Dannheim, MD, of Germany; and D. Peter Choyce, MD, FRCOphth, of London—the pioneers of intraocular implants—conducted the first trials using anterior chamber refractive lenses to correct high myopia in phakic eyes. Unfortunately, the initial experiments revealed unacceptable complication rates due to imperfections in IOL design.1 Glaucoma, corneal dystrophy, and hyphema were commonly observed, and anterior chamber implants—particularly refractive phakic implants—acquired a bad reputation.
EARLY PROTOTYPES
It was not until the mid-1980s that Svyatoslav N. Fyodorov, MD, of Moscow; Paul U. Fechner, MD, of Germany; and I resumed developing phakic implants.
Dr. Fyodorov began experimenting with a collar-button, pupil-fixated posterior chamber implant that ultimately led to the development of the Implantable Contact Lens (ICL; STAAR Surgical), the Adatomed implant (Chiron Adatomed), and the Phakic Refractive Lens (PRL; Ciba Vision). Dr. Fechner designed the Worst iris claw implant (Ophtec) and adapted it to correct high myopia. Later, Ophtec modified the implant to also correct hyperopia and astigmatism. I imagined an angle-supported implant to correct myopia similar to that designed by Charles D. Kelman, MD, of New York.
Over the last decade, the development of phakic implants has been erratic: first one type met with success, then another. In fact, the progress of these lenses was largely hindered by the importance of concurrent investment and research into corneal surgery, microkeratomes, and the excimer laser. Because LASIK developed so rapidly, today, its advantages and limitations are much better known. Due to the procedure’s drawbacks, interest and research in refractive implants are once again gaining momentum.
ADVANTAGES OF REFRACTIVE IMPLANTS
Apart from progressive myopia and cataract development, the stability of refractive results has been confirmed regardless of the implant type. Safety and efficacy ratios are superior to those obtained with LASIK, and optical aberrations are fewer.2,3 In most instances of high ametropia, the effective optical zone is larger, and the rate of nighttime halos is lower with refractive implantation versus corneal surgery. Additionally, fewer optical defects occur with industrial lens implantation compared with corneal surgery, because the ultimate shape of the corneal tissue depends on the individual’s healing ability. In most cases, refractive implant procedures are reversible. In the event of a sizing or power error, the lenses can be exchanged.
DISADVANTAGES OF REFRACTIVE IMPLANTS
The disadvantages of refractive implants depend on the lens model and its anatomical situation. Each new modification can induce an unexpected iatrogenous complication.
Angle-supported anterior chamber implants. Respecting a safety profile has eliminated the early endothelial trauma observed with the first models. To prevent endothelial loss, there must be a minimum of 1.5 mm between the edges of the optic and the endothelium. More than 80% of the first-generation (years, 1988–1989) ZB-type Baikoff phakic IOL implants have been extracted. Since 1990, and until last year, no known or published corneal dystrophy epidemic has been reported with new-generation implants.
Indeed, sudden drops in endothelial cells have been described in France, when the Vivarte (Figure 1) or Newlife lens (both manufactured by Carl Zeiss/IOLTech) was implanted in patients 4 or 5 years ago. During the first 3 or 4 years, the endothelial cell loss is physiological. A sudden drop in the number of endothelial cells occurred after the fourth year and led to explantations in 10% to 20% of cases. These implants were withdrawn from the market and a warning issued—not only with regard to these implants, but to all types of anterior chamber implants.
Figure 1. The Vivarte presbyopic phakic IOL.
In our experience, we have noted that second-generation PMMA implants (ZB5M [Domilens] or Nuvita [Bausch & Lomb]) presented few endothelial problems, and the average number of years before it was explanted (for whatever reason) was approximately 11 years. It was only 2 years with the Vivarte and Newlife. We were unable to find anatomical reasoning for the endothelial cell loss. Moreover, there did not seem to be any relationship between the anterior chamber depth and endothelial cell loss. We, therefore, wondered if it was a question of hydrophilic polymer tolerance in the anterior chamber.
The future of angle-supported implants lies in perfecting the preoperative evaluation of the anterior chamber’s internal diameter. Anterior chamber implants have followed the example of posterior chamber implants and may now be inserted through a 3-mm or smaller self-sealing incision.
Iris claw/iris-fixated implants. The complication rate of iris-fixated phakic IOLs has fallen. Endothelial cell loss is acceptable, and inflammation, pupillary blocks, and IOL displacements are rare. A few implant dislocations were observed when the IOL was not firmly fixed at the iris.2,3 Pigment dispersion has been noted in hyperopes,2,3 and I observed several cases—essentially in hyperopes and in one case in a myope—when I carried out a retrospective analysis of the anterior chamber on several hundred patients using the Visante OCT (Carl Zeiss Meditec). We were able to show that pigment dispersion always occurred when the crystalline lens rise was equal to or greater than 600 µm.1-6 The forward protrusion of the crystalline lens pushes the iris toward the front, creating a sandwich effect where the iris is squashed between the implant and the crystalline lens. At that moment, pigment dispersion syndrome occurs.
Therefore, we no longer offer iris-claw implants to patients if their crystalline lens height/rise is more than 300 µm. By keeping to this rule, we have been able to eradicate this problem from our practice. It is important to note, however, that the crystalline lens’ anterior pole moves forward by 20 µm per year. From 10 to 15 years on, we will once again be confronted with this problem.
To solve the large incision problem, a foldable version of the Artisan lens (Ophtec; marketed in the US as the Verisyse IOL by Advanced Medical Optics), called the Artiflex implant, is being developed.
Posterior chamber implants. Currently, surgeons prefer either the ICL or the PRL. The risk of cataract formation is still a problem, especially regarding the ICL. The rate increases with age and insufficient vaulting of the implant.4 Additionally, cases of unexplained intravitreous dislocations with the PRL have been recently published (oral communication with Dimitri Dementiev, MD, at the ESCRS Winter Meeting, Barcelona, Spain, February 2004). Whether this complication is due to surgical trauma, the cutting effect of the PRL’s edges or a fragile zonule is unknown. This complication has not been described with the ICL, which is sulcus-fixated.
THE FUTURE OF PHAKIC IMPLANTS
Today, phakic IOLs represent only a small part of refractive surgery indications. However, because of their optical qualities and their theoretical and practical advantages, as well as the contraindications and limitations of LASIK, I initially believed that these implants would make up approximately 20% to 30% of the refractive surgery market. Unlike what I thought some years ago, the market of phakic implants will probably not be as important as first estimated because of the adverse effects we have observed on all types of implants. Their usage will probably only cover 10% to 20% of refractive surgery indications.
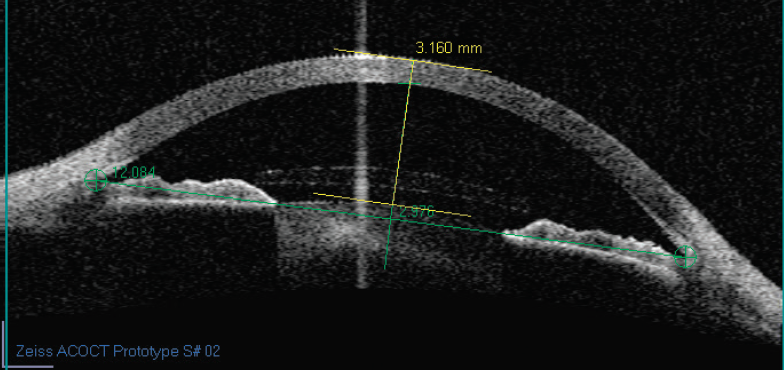
Figure 2. An anterior segment cut using anterior chamber OCT.
Our experience shows that the key to successfully using angle-supported implants is evaluating the anterior chamber’s internal diameter. Previously, measuring the external white-to-white measurement was imprecise. Today, however, axial imaging techniques that cover the entire diameter of the anterior segment such as the Scheimpflug technique, high-frequency ultrasonographs, and an optical coherence tomographer are in development (Figure 2). Their precision has a 50-µm variation. The software of these devices may shortly be capable of simulating the presence of an implant in the anterior segment, thus indicating whether or not the safety guidelines have been respected.
1. Baikoff G, Lutun E, Ferraz C, et al. Analysis of the eye’s anterior segment with an optical coherence tomography: static and dynamic study. J Cataract Refract Surg. 2004;30:1843-1850.
2. Baikoff G, Lutun E, Ferraz C, et al. Refractive Phakic IOLs: contact of three different models with the crystalline lens, an AC OCT study case reports. J Cataract Refract Surg. 2004;30:2007-2012.
3. Baikoff G, Bourgeon G, Jitsuo Jodai H, et al. Pigment dispersion and artisan implants. The crystalline lens rise as a safety criterion. J Cataract Refract Surg. 2005;31:674-680.
4. Baikoff G, Luntun E, Ferraz C, Wei J. Anterior chamber optical coherence tomography study of human natural accommodation in a 19-year-old albino. J Cataract Refract Surg. 2004;30:696-701.
5. Baikoff G, Rozot P, Lutun E, Wei J. Assessment of capsular block syndrome with anterior segment optical coherence tomography. J Cataract Refract Surg. 2004;30:2448-2450.
6. Baikoff G, Jodai H, Bourgeon G. Evaluation of the measurement of the anterior chamber’s internal diameter and depth: IOLMaster vs AC OCT. J Cataract Refract Surg. 2005;31:1722-1728.
The departures of these phakic lens technologies were due to a number of reasons, among them iatrogenic damage to the corneal endothelium or the crystalline lens, difficulty of implantation or fixation, and induced astigmatism due to the large incisions needed for implantation of rigid PMMA IOLs. These issues have been largely addressed through incremental improvements over the decades, and in 2018, two major designs endure (see Today’s Phakic IOLs).
TODAY’S PHAKIC IOLS
IRIS-FIXATED
• Originally called the Worst iris-claw phakic IOL (Ophtec)
• Now known as the Artisan (Ophtec) in Europe and the Verisyse (Johnson & Johnson Vision) in the United States, and their foldable cousins, the Artiflex (Ophtec) in Europe and the Veriflex (Johnson & Johnson Vision) in the United States
POSTERIOR CHAMBER
• Originally known as the Implantable Contact Lens (STAAR Surgical)
• Most recently called the EVO Visian ICL (STAAR Surgical)
According to Market Scope data, in 2016, the Visian ICL (STAAR Surgical) accounted for approximately 62% of the global market for phakic IOLs, and the Artisan/Verisyse and Artiflex/Veriflex (Ophtec/Johnson & Johnson Vision) lenses together accounted for approximately 36%. There are other phakic IOLs still on the market, but they made up only about 2% of the total global market, according to that 2016 data.
Indications for phakic IOL implantation (Figure) have also changed over the decades. Dr. Baikoff noted that they were originally indicated only for patients with very high ametropias, but phakic IOLs are now used in patients with lower degrees of error as well. On top of this, they may be appropriate for patients who are contraindicated for LASIK or PRK because of corneal abnormalities or dry eyes. Indications for the iris-fixated models depend on the dimensions of the anterior chamber, as sufficient depth is required to avoid endothelial touch.
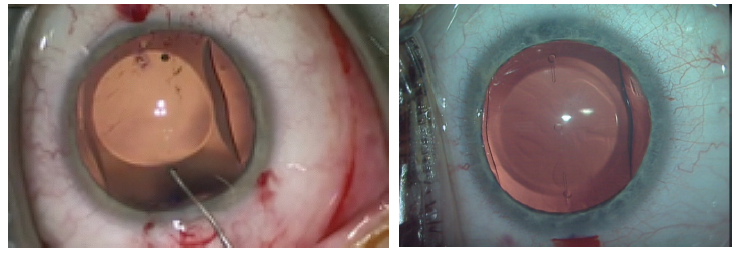
Figure. The Visian ICL being implanted (left) and in situ (right).
COMPARISONS
Kobashi and coauthors1 compared quality of life following Visian ICL implantation in patients with mean preoperative manifest refraction spherical equivalent (MRSE) of -9.97 ±2.51 D (range, -3.00 to -14.50 D) to that following LASIK in patients with mean preoperative MRSE of -6.31 ±2.20 D (range, -3.00 to -12.88 D). They reported that scores for activity limitations, symptoms, appearance, and satisfaction with correction were significantly higher in the phakic IOL group than in the LASIK group. The authors concluded that long-term vision-related quality of life advantages with the Visian ICL included fewer activity limitations and symptoms and better appearance and satisfaction with correction compared with myopic wavefront-guided LASIK.
A multicenter Japanese study recently assessed the results of currently used refractive surgical procedures, including phakic IOLs, in more than 15,000 eyes.2 The study by the Survey Working Group of the Japanese Society of Cataract and Refractive Surgery included patients who underwent LASIK, excimer laser surface ablation, refractive lenticule extraction, or posterior chamber or iris-supported phakic IOL implantation at one of 42 major institutions.
In brief, at 3 months postoperative, these authors found that 99% of patients with posterior chamber phakic IOLs and 84% with iris-supported phakic IOLs achieved within ±1.00 D of attempted correction. This compared with 96% for LASIK, 93% for surface ablation, and 97% for refractive lenticule extraction. The authors concluded that all of these approaches to refractive surgical correction “have good safety and efficacy outcomes, yielding predictable and stable results [and] appear to be feasible options for the treatment of refractive errors.”2
The possibility of providing substantial gains in quality of life for our patients creates a strong incentive for surgeons to consider phakic IOL implantation.
FUTURE PROSPECTS
Today, the long-term safety and effectiveness of current phakic IOL models is well established. Regarding the ICL in particular, there have been more than 900,000 implants to date, and some ICLs have now been in patients’ eyes for more than 20 years.
The history continues to unfold, as STAAR Surgical received US FDA approval earlier this year for the Visian Toric IOL—the first toric phakic IOL to be approved in the US market. The Visian Toric has been approved for use in Europe since December 2002, and toric versions of the Artisan and Artiflex are also available in Europe.
In this era of aging baby boomers, it is worth noting that phakic IOLs work with the patient’s residual accommodation, preserving the cornea and lens for future procedures. The lenses are removable, and, therefore, reversible if other options to address a patient’s change in refractive status become available.
It is safe to say that phakic IOLs are now a familiar and versatile tool in the refractive surgeon’s toolkit, and they are likely to be with us for many years to come.
1. Kobashi H, Kamiya K, Igarashi A, Matsumura K, Komatsu M, Shimizu K. Long-term quality of life after posterior chamber phakic intraocular lens implantation and after wavefront-guided laser in situ keratomileusis for myopia. J Cataract Refract Surg. 2014; 40(12):2019-2024.
2. Kamiya K, Igarashi A, Hayashi K, Negishi K, Sato M, Bissen-Miyajima H; Survey Working Group of the Japanese Society of Cataract and Refractive Surgery. A multicenter prospective cohort study on refractive surgery in 15 011 eyes. Am J Ophthalmol. 2017;175:159-168.
