




A lot has happened since Sekundo and Blum introduced the advantages of small-incision lenticule extraction (SMILE) at the 2006 AAO Annual Meeting1 and wrote about the procedure in CRST Europe (see accompanying excerpt below). At that time, they referred to the procedure as femtosecond lenticular extraction, or FLEx.
An excerpt from CRST Europe April 2007
Femtosecond Lenticular Extraction
This investigational new procedure is unique to the VisuMax laser and currently performed by only two clinical investigators in Germany.
By Walter Sekundo, MD
I am a clinical investigator of a new technique called femtosecond lenticular extraction (FLEx). This new innovation in corneal laser surgery uses a femtosecond laser alone, compared with other procedures that use an excimer plus femtosecond laser.
Marcus Blum, MD, of Erfurt, Germany, and I introduced FLEx at the 2006 American Academy of Ophthalmology Annual Meeting, in Las Vegas. Although the procedure is not yet approved, FLEx has demonstrated the enormous potential of VisuMax (Carl Zeiss Meditec), because the quality of cut allows us to extrude the refractive lenticule from the cornea. The following information provides an account of how the procedure works.
FLEx is not LASIK; the healing responses of the two procedures are quite different. For instance, there is no initial overcorrection as seen with the excimer laser. The cornea is not ablated during FLEx like it is when an excimer laser is used. Therefore, energy is not lost at the periphery of the ablation, and prolate refractive zones are similar to wavefront-optimized excimer laser ablation results. Our results with FLEx, which is a single-step procedure (Figure), are much better than we ever expected.
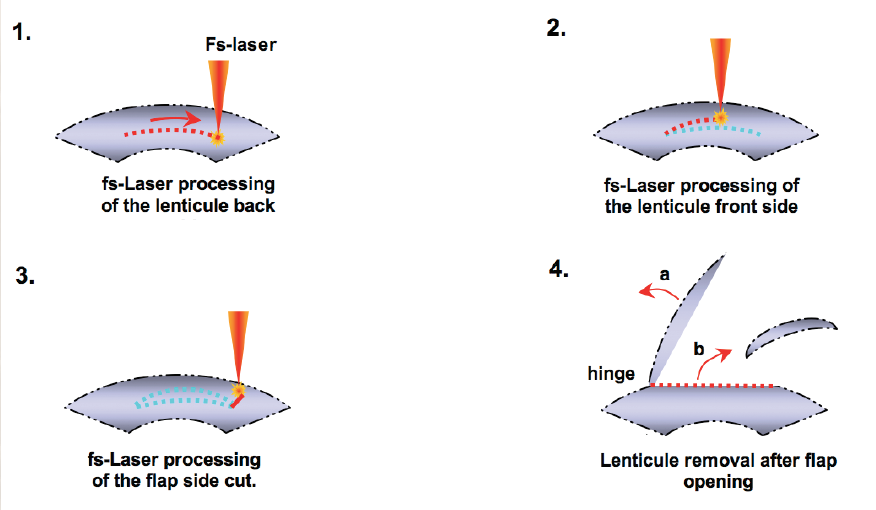
Figure. FLEx is a single-step procedure.
HOW IT WORKS
During FLEx, the femtosecond laser creates a refractive and a nonrefractive cut in a single step. After the flap is lifted, a piece of stromal corneal tissue (ie, refractive lenticule) is removed. Next, the flap is repositioned in the usual fashion. This new procedure has an enormous potential. Currently, we have 3-month results; however, Carl Zeiss Meditec will soon release the 6-month follow-up data. At 3 months, all patients treated with FLEx were 20/40 or better uncorrected. If we can customize and further improve upon the FLEx procedure, surgeons could conduct an entire lamellar refractive procedure with the femtosecond laser alone.
MY EXPERIENCE
The final version of the VisuMax femtosecond laser was released for clinical validation in February. We have treated 32 myopic eyes using the VisuMax/MEL-80 platform (Carl Zeiss Meditec). The results have been spectacular; a few patients have experienced 20/10 uncorrected vision 1 day following surgery. I have cut very thin flaps as well as thick flaps (range, 100–150 µm). In the more than 50 procedures I have performed so far, I have never created a buttonhole, tear, or any other complication that one experiences with normal microkeratomes.
We expect a further intense phase of clinical research before this procedure might become commercially available; however, FLEx has the potential to revolutionize the entire course of corneal refractive surgery. This is the fascinating procedure of the future.
Since then, more than 1.5 million SMILE procedures have been performed worldwide, and an abundance of scientific data has demonstrated the clinical advantages of this minimally invasive approach to refractive surgery.2,3 (Editor’s note: SMILE can currently only be performed with the VisuMax femtosecond laser [Carl Zeiss Meditec]; however, two related procedures are being studied by Schwind eye-tech-solutions and Ziemer. For more information on those techniques, see On the Horizon at the bottom of this article.) I started performing SMILE 6 years ago, and in that time, I have observed significant clinical improvements with the procedure in comparison with femtosecond LASIK (see Reasons to SMILE).
REASONS TO SMILE: DR. BREYER’S CLINICAL COMPARISON WITH FEMTOSECOND LASIK
• We see almost no dry eyes after SMILE, which is a major clinical advantage over LASIK because many patients who come to see us for refractive surgery cannot wear contact lenses due to dry eyes.
• There are no flap complications with SMILE, such as folds or dehiscence, because the procedure does not require a flap. Many patients expressed reluctance to undergo laser vision correction in the past because of the possibility of flap complications. They are happy now to hear that there is a flapless method.
• In many cases, SMILE can be performed with a cap 150 µm deep, leaving the upper part of the cornea nearly untouched. As this part of the cornea imparts most of the cornea’s strength, it is hoped that this will decrease the risk of late keratectasia.
• For the first time, we have a laser vision correction procedure that is completely painless intra- and postoperatively, according to my patients’ feedback. This further reduces patient reluctance to undergo the procedure, as fear of pain was another major factor preventing patients from undergoing laser vision correction in the past.
• The excellent quality of vision after SMILE, due to the smooth, wide optical zone, has significantly reduced postoperative complaints from patients regarding photopic phenomena during nighttime driving after laser vision correction.
• The comfort and safety level for patients directly after SMILE surgery is another advantage. Rubbing the eyes immediately after surgery is without risk. We allow patients to participate in sports, to use makeup, and to take a shower the same day as surgery. No eye shields are needed overnight, as they are in LASIK, so patients can sleep well (and so can the doctor).
EXPANDING INDICATIONS, IMPROVED HARDWARE
In October, Carl Zeiss Meditec received US FDA approval of SMILE for myopic astigmatism, further extending the treatment options for patients in that part of the world. But what about the treatment of hyperopia? Early clinical results from Dan Z. Reinstein, MD, MA(Cantab), FRCSC, DABO, FRCOphth, FEBO, and Walter Sekundo, MD, suggest good outcomes.4,5
Is there a need to improve the hardware and laser settings for SMILE? Iris recognition and eye tracking capabilities for the correction of astigmatism are desired more by LASIK-only users than by SMILE users. The latter have fine-tuned their visual acuity outcomes by creating and perfecting individual nomograms. We recently presented our own results with SMILE at the ESCRS and ASCRS meetings, including our low retreatment rate of only 0.3% (Figure).6,7
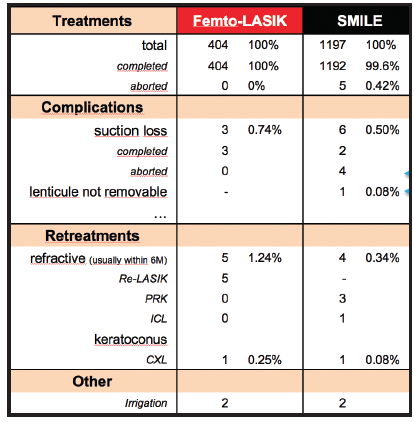
Figure. Comparison of complications and retreatment rates after SMILE and femtosecond LASIK at Dr. Breyer’s clinic.
A trend toward use of low-energy settings has improved visual acuity results on day 1 postoperative. Donate and Thaeron conducted a study assessing early visual and optical quality recovery after SMILE using laser energy level settings close to the plasma threshold. They found that this approach had minimal effect on ocular scatter and achieved better and faster visual recovery in patients with moderate myopia.8 Nearly all of our ReLEx SMILE patients can drive a car on postoperative day 1 with binocular UCVA of 20/20.
RECYCLING THE LENTICULE
Is the lenticule we extract in SMILE just a waste product, or can it be meaningfully reused? Several recent studies suggest that the answer is the latter.
Klimesova et al found that corneal tissue lenticules could be safely and effectively used to correct keratoconus, and they suggested that this may be considered as an alternative method to prevent or delay keratoplasty in these patients.9 Ganesh and Brar recently reported 2-year results with this technique, in which a femtosecond laser pocket is created in the hyperopic patient’s cornea, and a cryopreserved or fresh lenticule, obtained from a myopic patient undergoing SMILE and matched for refractive error, is implanted.10 Zhou and Li investigated the safety and efficacy of tissue addition for post-LASIK keratectasia by implanting a hyperopic lenticule in the stromal bed after lifting the flap. These authors concluded that the implantation of an allogenic lenticule may be an option in the treatment of post-LASIK ectasia.11
CONCLUSION
In our practice, SMILE has nearly replaced LASIK in the correction of myopia from -1.00 to -10.00 D, and it has raised patient satisfaction to a high level. SMILE is accepted much more readily by patients than LASIK, and I am sure that its popularity will continue to grow.
On the Horizon
Two new lenticule extraction procedures not yet available have thus far produced promising results.
By Theo Seiler, MD, PhD; and Christian Rathjen, PhD
Schwind’s Lenticule Extraction Procedure
By Theo Seiler, MD, PhD
Schwind eye-tech-solutions has developed a corneal lenticule extraction procedure comparable with the small-incision lenticule extraction (SMILE) technique introduced by Carl Zeiss Meditec. In my opinion, however, the Schwind technique is smarter, and the learning curve is significantly shorter.
The repetition frequency of the new Schwind femtosecond laser is currently 2 MHz, but it can be tuned up to 10 MHz. The cutting pattern is more intelligent because it does not need the cylindrical cut at the edges as used in SMILE. In consequence, this leads to less healing response. The curvature of the new patient interface is stronger compared with the VisuMax femtosecond laser (Carl Zeiss Meditec), resulting in fewer intrastromal surface irregularities. Cyclotorsion control and eye-tracking technology will be utilized in the Schwind lenticule extraction procedure.
The proposed Schwind lenticule extraction procedure will use two small incisions, 90° away from each other, one incision leading to the anterior surface and the other to the posterior surface of the lenticule. This will make the procedure easier and the learning curve shorter.
In India, we performed the procedure for the first time in a series of patients (N = 20) in order to establish nomograms and improve parameters. In the first group of patients, we had significant undercorrection, but in a second group the undercorrection rate was as low as 5%. When I did these procedures in India, my personal impression was that the procedure is easier to perform compared with the SMILE procedure.
During brainstorming seminars, we are already planning customized treatments based on topography or wavefront analysis. With the built-in cyclotorsion and eye-tracking technologies, the results of correction of myopic astigmatism will be significantly improved, comparable to the improvement that cyclotorsion and eye tracking brought to LASIK 15 years ago. (It is high time that these technologies were brought to SMILE.)
To the best of my knowledge, Schwind eye-tech-solutions is expecting to apply for the CE Mark for the device in spring 2019, and, therefore, I assume that it will be available on the market at earliest by the second quarter of 2019.
Ziemer’s Lenticule Extraction Procedure
By Christian Rathjen, PhD
Still in the developmental phase and in response to trends in today’s corneal refractive surgery market, Ziemer is working on a lenticule extraction procedure that will be performed with the company’s Femto LDV Z8 femtosecond laser. This procedure will apply the same low-energy principle used by the laser during LASIK and other corneal procedures, but it will incorporate a new scanning algorithm to execute the lenticule extraction procedure.
Before I share preliminary information on this procedure, I want to make it clear that, as a company, Ziemer strongly believes that LASIK is alive and well. This new lenticule extraction procedure is not meant to replace or be an upgrade to LASIK or even PRK, but rather an alternative that surgeons can choose to perform when appropriately indicated in their patients. We are still very much in favor of modern LASIK because of its outstanding safety and performance; however, in certain markets, lenticule extraction seems to be a valuable supplement to the refractive surgeon’s portfolio.
With that said, we are excited by the potential of Ziemer’s new lenticule extraction procedure. For the past 6 months, we have been working with three surgeons to gather early hands-on experience. The feedback we have received regarding the overall quality and precision of the scanning algorithm and the lenticule extraction procedure is encouraging enough to continue our development. To date, surgeons have seen the same cut quality in these lenticule procedures as in LASIK femtosecond flaps performed with the Femto LDV.
We expect to present data on the procedure at meetings in the coming year, and we plan to make the first software module available for experienced corneal surgeons. Initially, the refractive indication will be for the treatment of myopia.
1. Sekundo W. Femtosecond lenticular extraction. CRST Europe. April 2007.
2. Reinstein DZ, Archer TJ, Gobbe M. Small incision lenticule extraction (SMILE) history, fundamentals of a new refractive surgery technique and clinical outcomes. Eye Vis (Lond). 2014;16(1):3.
3. Kobashi H, Kamiya K, Shimizu K. Dry eye after small incision lenticule extraction and femtosecond laser-assisted LASIK: Meta-analysis. Cornea. 2017;36(1):85-91.
4. Reinstein DZ, Pradhan KR, Carp GI, et al. Small incision lenticule extraction (SMILE) for hyperopia: Optical zone centration. J Refract Surg. 2017;33(3):150-156.
5. Reinstein D, Carp G, Archer T, Dhungana P, Khan R. SMILE for hyperopia: Visual and refractive outcomes at 3 months. Paper presented at: the 35th Congress of the ESCRS; October 7-11, 2017; Lisbon, Portugal.
6. Breyer D. Five-year results of refractive lenticule extraction ReLEx SMILE compared to femto-LASIK. Paper presented at: the 36th Congress of the ESCRS; September 22-26, 2018; Vienna, Austria.
7. Hagen P. Impact of biomechanical indices on visual outcome up to five years after refractive lenticule extraction (ReLEx) SMILE. Paper presented at: the 36th Congress of the ESCRS; September 22-26, 2018; Vienna, Austria.
8. Donate D, Thaeron R. ReLEx SMILE with low energy levels: Assessment of early visual and optical quality recovery. Paper presented at: the 36th Congress of the ESCRS; September 22-26, 2018; Vienna, Austria.
9. Klimesova Y, Studeny P, Magdalena N. Corneal tissue lenticules from ReLEx SMILE for the correction of keratoconus: Case reports. Poster presented at: the 36th Congress of the ESCRS; September 22-26, 2018; Vienna, Austria.
10. Ganesh S, Brar S. Long-term safety, visual, and refractive outcomes after femtosecond laser intrastromal lenticule implantation for treatment of hyperopia. Poster presented at: the 36th Congress of the ESCRS; September 22-26, 2018; Vienna, Austria.
11. Zhou X, Li M. Tissue addition for post-LASIK ectasia by implanting a lenticule after SMILE. Paper presented at: the 36th Congress of the ESCRS; September 22-26, 2018; Vienna, Austria.
