



This year has seen a great deal of debate regarding keratoconus and CXL. A number of key questions have been raised—and many have been answered. (For a historical perspective on the development of CXL, see the accompanying excerpt starting below.)
An excerpt from CRST Europe January 2011
The Future of Corneal Collagen Crosslinking
Key opinion leaders addressed benefits of this state-of-the-art treatment during a roundtable discussion held at the 2010 ESCRS meeting in Paris.
By Arthur B. Cummings, MB ChB, FCS(SA), MMed(Ophth), FRCS(Edin); Sheraz M. Daya, MD, FACP, FACS, FRCS(Ed), FRCOphth; A. John Kanellopoulos, MD; Antonio Leccisotti, MD, PhD; Michael Mrochen, PhD; Roy S. Rubinfeld, MD; Theo Seiler, MD, PhD; Aleksander Stojanovic, MD; and William B. Trattler, MD
Trattler: Gathered here are some of the leaders in CXL. The purpose of our discussion is to recap the history of CXL and explore how it is being used in refractive surgery today. By the conclusion of this roundtable, we will have highlighted our preferred techniques; overviewed the indications, contraindications, and complications; and provided rationales for the use of CXL as both standalone and combined treatment modalities.
THE EPITHELIUM
Rubinfeld: Let’s be sure we are all speaking the same language. Are you doing CXL with the epithelium on or off?
Daya: Epithelium on, but I use a disruptive device (the Daya Disruptor; Duckworth & Kent) to create pockmarks in the epithelium. The primary goal is to maintain as much live epithelium as possible but also promote riboflavin penetration—and it does penetrate. The secondary goal is to reduce inflammation in the eye and to get the patient out of the contact lens within 24 to 48 hours.
Some surgeons have noticed increased astigmatism and refractive change following CXL when the epithelium is removed, but in my experience this is not the case when the epithelium is left intact. With our epithelium-on method using the disruptive device, demarcation lines signify where the riboflavin penetrates the anterior cornea. The great thing is that patients do not have a huge refractive change for the worse; it either stays the same or improves. Sometimes they get a bit of induced astigmatism, but only for 1 to 3 months.
Trattler: How long do you saturate the eye with riboflavin?
Daya: Approximately 30 to 45 minutes.
Trattler: Roy and I are working together on a multicenter CXL outcomes study in the United States. About 4 months ago, we both converted from 100% epithelium-off to epithelium-on (ie, transepithelial) treatments. We leave the riboflavin drops in the eye for approximately 60 to 90 minutes, gauging when there is enough riboflavin penetration. We have seen some very nice early results.
Seiler: It must be said that 4 months is not long enough to establish solid evidence. Ideally, 1-year data from a controlled study would be preferable.
Kanellopoulos: I would like to stay on the topic of controlled studies. What Theo says is valid. The problem is, however, when we do a controlled study, what are we measuring? One of the most painstaking things for us, clinically, is to find a measurement aside from corneal curvature to assess the effects of CXL.
Seiler: I fully agree. In the early days, we thought that we were stuck with the experimental setup of crosslinking in strips and measuring whether the strip became stiffer. As long as there are no data, I am not willing to accept that as solid proof that a CXL protocol works. One surgeon may crosslink only 55% of the cornea effectively, but he or she happens to be treating patients who do not require 100% crosslinking. The same protocol will not work for the surgeon who is treating advanced keratoconus with CXL. The bottom line is that each surgeon must provide data and be honest as a scientist.
Roberto Pinelli, MD, of Brescia, Italy, uses an epithelium-on approach. When we used his treatment protocol, we found that not one single keratocyte was killed. This means that not one single cell membrane of the keratocytes was crosslinked, and that means the treatment was ineffective. Nevertheless, patients could not perceive any difference, except that they did not feel pain. We now use a different epithelium-on approach, and this seems to work better for us.
Rubinfeld: Is apoptosis required for crosslinking?
Seiler: That is exactly the crucial point. It might well be, and that was our previous approach. But with our current approach of epithelium off we are just doing an overkill when we crosslink 100%. The best guess for the epithelium-on approach is 20% to 50% of the epithelium-off effect. Two years ago, we determined that the failure rate after standard CXL was 3% as long as we stayed away from eyes with advanced keratoconus and treated only eyes with a maximum keratometry (K) reading of less than 58.00 D. I assumed the failures were because of measurement errors, and so I did a full treatment. But when crosslinking was reduced by 80%, results did not look similar. Maybe what we need to do next is reduce the time step by step, for example, to see what that would do to the failure rate. Then we would know whether we are at the upper limit for crosslinking and whether we can reduce it.
HOW MUCH CXL?
Rubinfeld: I’d like to go back to Theo’s question. If you need only 50% crosslinking, can you still get good results with not as much CXL?
Seiler: Possibly; it is only speculation.
Rubinfeld: How much CXL do we want? Is there a problem with crosslinking everyone to 100%?
Mrochen: But first, what do we mean by 100%?
Rubinfeld: I don’t know. Biochemically, what happens? I know that crosslinking links two entities; however, can we link them all, and do we want to?
Kanellopoulos: We are unsure. It may be that CXL just shrinks collagen but does not interlink the collagen fibers.
Seiler: We originally thought we were creating interfibrillar crosslinks, but we are no longer sure. We know with certainty that crosslinks are induced inside the fibrils. It might be that proteoglycans induce some interfibrillar crosslinks, but that is not proven.
Rubinfeld: If I can ask my question again, even less intelligently than the last time: Whatever crosslinking is…
Seiler: Very well said.
Rubinfeld: …do we want a lot of it, or do we want some of it?
Daya: I think it varies based on other variables, such as how severe the keratoconus is, how elastic the cornea is, and the age of the patient.
Rubinfeld: Is there harm in doing as much CXL as possible?
Mrochen: We did animal studies together with the University of Belgrade (Schumacher S, Jankov M, Bueeler M, Simon D, unpublished data, 2010) in which we looked at the intensities and concentrations of CXL. We believe that there is a certain limit over which the result is a lot of scarring that appears as large whitish spots. We call this over-crosslinking.
Seiler: You can also get agglomerations of collagen when you reach the upper limit of crosslinking. If you do too much it comes at a certain expense (eg, white plaques).
Rubinfeld: Is there a limit of UV-A exposure?
Mrochen: We must be sure that there is always a correlation between UV-A intensity, time (which gives us the amount of energy to be applied and the number of photons), and the concentration of the riboflavin.
LOCALIZED TREATMENT
Kanellopoulos: It is not only a matter of how much crosslinking is needed but also where in the cornea it is needed. This varies for different corneal models. For a thicker, more normal cornea, which is a better biological model, much less crosslinking is needed. For an advanced keratoconus model, where everything is focused at one part of the cornea, more crosslinking is needed.
Therefore, when I perform CXL I focus on where the crosslinking is needed rather than how much, because that can be titrated. Theoretically, you can do three CXL procedures in the same patient, performing the second session 1 month after the first, and a third later if needed. The question is: What part of the cornea do we want to crosslink?
Rubinfeld: So you are suggesting selective crosslinking.
Seiler: Do we crosslink or not? This is not a yes-or-no question. We certainly know that strengthening the cornea is important, and we know that some corneas need more strengthening and others need less. We have to learn to titrate this effect over the long term to produce any answers.
COMBINED TREATMENTS
Kanellopoulos: Our Athens Protocol combines laser with CXL. We have not had any cases of breakthrough ectasia in a series of more than 400 cases. We compared 127 eyes treated with CXL first and topography-guided PRK later versus 198 that had the combined same-day treatment.1-3 None of the patients had breakthrough ectasia in more than 5 years’ follow-up. We concluded that crosslinking works no matter what the sequence.
Leccisotti: Is it OK to ablate a crosslinked cornea?
Kanellopoulos: That was the argument of the study. The answer is yes, it is OK.
Seiler: Strategically, it would be better to do PRK first and CXL afterward, because you can be sure that it is a fully crosslinked cornea. This will alleviate the possibility of removing what was the strongest part.
Cummings: Corneas that have been crosslinked are better-shaped corneas.
Seiler: On the other hand, some surgeons have argued that if PRK is done first in a weak cornea, the result is an immediate elastic response, steepening the periphery and flattening the center (or vice versa). They believe that this freezes the wrong shape with the CXL; however, John showed clinically that is not the case.
Kanellopoulos: They actually have a synergistic effect when you do the procedures together. I want to go on the record saying that, in these eyes, PRK is a therapeutic procedure. Perhaps the most important way that it works is not for refractive correction but for producing a better biomechanical model of the cornea. Ectasia is spread over a wider area, bringing balance to the cornea. It might help to do a hyperopic treatment to thin some of the peripheral cornea and redistribute the strain from blinking or intraocular pressure. This is one of the ways that the Athens Protocol works. However, I do not want to give surgeons the wrong impression; this is not a refractive procedure. We aim for 20/40 BCVA, but we also discuss the options of ICRS and corneal grafts with patients.
ONGOING CHANGES AFTER CXL
Rubinfeld: Why are clinical results better at 4 years than they were at 1 year if you do only CXL?
Kanellopoulos: The tissue and the cornea are reexpanding. The periphery of the cornea expands more than the center, and the result is flattening.
Seiler: We have patients in Zurich with 5-year follow-up who have shown constant change. Some patients we treated had extreme thinning of the superior cornea close to the limbus. Over the course of 2 years, the peripheral cornea continued to get thicker; we believe that the collagen is out of equilibrium between synthesis and catalysis. These changes are not only biomechanical, they are also biochemical.
Cummings: Crosslinking may be a drug after all.
Daya: Keep in mind that this is all speculative.
Seiler: The augmentation has been documented, however.
Daya: Absolutely. But the reason why the cornea keeps changing, whether it be biomechanical or biochemical synthesis and degradation, is yet to be proven. Bone takes about 30 years to turn over. Who knows how long it takes cornea to turn over?
PROGRESSION AND RETREATMENT
Rubinfeld: Can CXL be repeated?
Daya: The only times we have done repeated CXL are in patients with post-LASIK ectasia. It seems to arrest development. The first CXL slowed progression, but the ectasia started to progress again. As a last-ditch effort before grafting, I performed CXL a second time.
Seiler: We and others have published results from cases of women who developed ectasia whenever they became pregnant.4 In one case, we performed CXL after the first pregnancy, but during subsequent pregnancies they developed ectasia again due to hormonal changes. In this instance, results were stable for 5 years, but when this woman became pregnant, suddenly the keratectasia occurred.
DEFINING CONCENTRATIONS, DOSING
Kanellopoulos: I have tested different concentrations of riboflavin, and increasing the concentration from 0.01% to 0.02% increases tenfold the crosslinking reaction (unpublished results). Using 0.05% riboflavin and crosslinking with 7 mW/cm2, you get a tremendous amount of crosslinking, but the corneas turn white. There must be some element in the procedure that increased the fluence of UV-A light or increased the effective concentration of riboflavin.
Seiler: We have found that when reducing the irradiation time by half you must triple the intensity.
Trattler: If you apply drops for 15 minutes versus 30, then you change the amount of riboflavin in the cornea. Is the type of riboflavin and the dosing that you put in more important than the concentration? As I understand it, more riboflavin in the cornea produces more crosslinking.
Kanellopoulos: Not necessarily, because the additional riboflavin shields more UV-A light.
Seiler: Superiorly you get more.
Kanellopoulos: And less inferiorly.
Mrochen: If you increase the concentration and use the same energy dose, you get a small layer of crosslinks.
Seiler: The links are shallower with a higher concentration of riboflavin.
Mrochen: If you want to extend that to deeper stroma, you must increase the energy dose, which means either increasing the intensity or the treatment time. Both might have an impact on the damage thresholds of the endothelium.
Trattler: Could you use less riboflavin?
Mrochen: Yes, because with 0.3% riboflavin, the crosslinks will be generated in deeper layers when the amount of energy in the cornea is increased. However, energy is also increased across the superficial layer, and we are afraid of over-crosslinking and generation of white superficial scars. We must determine the optimal balance among concentration, intensity, and time with respect to the endothelium and possible scarring that might occur.
Seiler: That is how we decided the original protocol of 30 minutes and 3 mW/cm2.
PATIENT SELECTION
Trattler: What population is appropriate for CXL? What are the limits for age, K readings, and corneal thickness?
Leccisotti: In Italy, our parameters are dictated by the National Health Service. It is reimbursed if the patient’s age is between 12 and 39 years and if the disease is progressing.
Trattler: But does it work in 40-year-olds? Do you see improvement in patients who are 40 or even 50 years old?
Cummings: I think if you have good indications, yes. I have done CXL in a couple of 55-year-olds who have had fantastic results.
Daya: Why did you treat them?
Cummings: Because they were progressing. The greatest effect of CXL is to stop progression.
Seiler: I would like to tell you the story of little Ioannis. He rubbed his eyes a lot, and after therapeutic treatment of the allergy there was still progression. Because he was a student, we decided to do CXL in the worse eye over his winter holiday and the fellow eye before the summer so he would not miss school. He came back in May with hydrops in the better eye. That has now made us suspicious about age limits and other variables.
Trattler: So age affects progression. That is useful information. Thank you all for participating in this roundtable discussion. CXL is an exciting treatment, and I have a feeling we will be seeing increased use over the next few years.
1. Kanellopoulos AJ. Post-LASIK ectasia. Ophthalmology. 2007;114(6):1230.
2. Kanellopoulos AJ, Binder PS. Collagen cross-linking (CCL) sequential topography-guided PRK: A temporizing alternative for keratoconus to penetrating keratoplasty. Cornea. 2007;26(7):891-895.
3. Kanellopoulos AJ. Comparison of sequential vs same-day simultaneous collagen cross-linking and topographyguided PRK for treatment of keratoconus. J Refract Surg. 2009;25:812-818.
4. Padmanabhan P, Radhakrishnan A, Natarajan R. Pregnancy-triggered iatrogenic (post-laser in situ keratomileusis) corneal ectasia-A case report. Cornea. 2010;29(5):569-572.
AREAS OF STUDY WITH KEY QUESTIONS ANSWERED
Thin corneas. Deciding what to do with thin corneas is a challenge. The Dresden protocol recommends treating only corneas thicker than 400 µm to prevent endothelial damage.1 Current approaches to treating thin corneas include the use of hypoosmolar riboflavin and contact lens–assisted CXL. However, swelling after application of hypoosmolar riboflavin changes the hydration state of the cornea and may affect the outcome. And the same is true of contact lens–assisted CXL because the first 200 µm of crosslinked tissue receives the greatest effect, and we end up crosslinking more contact lens than stroma.
However, if we return to CXL’s first principles—UV-A light, irradiation time, oxygen, and riboflavin concentration2—we may be able to build a validated model of how these factors combine to stiffen the cornea. With this tool in hand, should we not be able to determine how deeply CXL will affect the corneal tissue in every individual cornea? If so, a personalized irradiation profile, based on the thickness of each individual cornea,3 could be created (Figure).
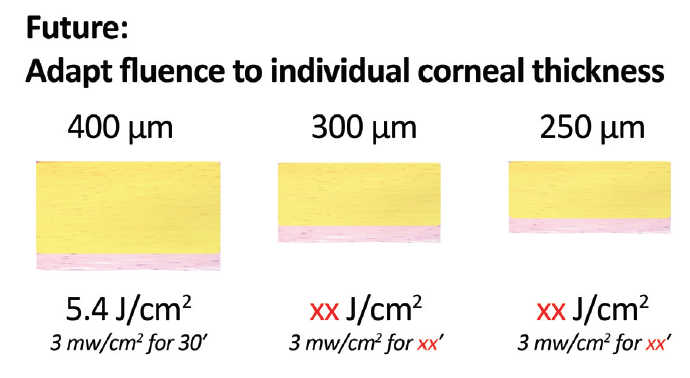
Figure. In the future, it might be possible to adapt fluence to individual stromal thickness, as it presents after the instillation of riboflavin.
Children. Progressive keratoconus is more prevalent and aggressive in children than in adults.4 The controversial question, therefore, is whether a child should be treated immediately or not treated until there are signs of progression. Multiple clinical studies of CXL in children have now been performed, and all have shown keratometric improvement or stabilization.5 The conclusion? Don’t wait. If any of my children were to have keratoconus, I would treat them immediately.
Infectious keratitis. Phagocytes in the immune system kill pathogens with reactive oxygen species (ROS). The photochemical reaction in CXL also creates ROS, happily with the same antiinfective effect.6 When used as a treatment for infectious keratitis, the procedure is called photoactivated chromophore for keratitis CXL (PACK-CXL).
PACK-CXL treatment does not have to follow the low-intensity Dresden protocol to be effective. Photochemical reactions are governed by the Bunsen-Roscoe law of reciprocity,7 which states that one achieves the same photochemical effect with a reduced irradiation time and increased radiation intensity, as long as the total dose remains the same. In other words, doubling the dose of light halves the time needed to perform CXL. This law makes one big assumption: All substrate molecules in the reaction are available in excess. In regular CXL for keratoconus, oxygen availability in the stroma limits this law,8 and we have shown that, with accelerated irradiation for less than 10 minutes duration, there is a reduction in crosslinking effect.
PACK-CXL, on the other hand, remains effective in treating antibiotic-resistant corneal ulcers even when accelerated protocols are used.9 Perhaps the antimicrobial effect may be partly independent of oxygen.
Despite differences from the Dresden protocol, PACK-CXL still manages to crosslink and strengthen the cornea, and these crosslinks are sufficient to increase resistance against enzymatic digestion.10 In a multicenter clinical trial, all patients enrolled in the study who have been treated with only PACK-CXL have not required additional antimicrobials to achieve epithelium closure (Hafezi, unpublished data).
Hormones. We’ve known since the first reports of post-LASIK ectasia in pregnant women that estrogen increases the elasticity of the cornea.11 Recently, our team studied corneal topographic changes in healthy pregnant women and found that the strongest correlation between topographic changes and hormone levels was not with estrogen but rather with thyroid hormone.12
Epidemiologic studies have shown that hypothyroidism and keratoconus are closely linked: If a patient has one of these disorders, it’s advisable to have him or her investigated for the other.13 I predict, therefore, that we will see studies in the near future that will take a closer look at thyroid hormones and CXL.
WHAT’S HEATING UP
CXL and wavefront-guided PRK can be combined to improve the corrected vision of patients with keratoconus. However, there is still room for improvement in how to perform this treatment. We now know that approximately 12% more energy is required to create any given ablation depth in a crosslinked cornea than in a noncrosslinked one,14 and laser manufacturers have begun to change their algorithms accordingly. The next challenge is how to address and to minimize laser ablation–induced corneal inflammation.15
A lot of refractive laser surgery involves physics, and so, prior to surgery, we pay attention to parameters such as laser repetition rate, power, spot size, and spot profile. But we seem to forget about the biology, other than separating beam spots sufficiently to avoid overheating the cornea. After surgery, on the other hand, everything is viewed from a biological standpoint: the wound healing response, the use of mitomycin C to prevent haze formation, and so on. We must begin to bring a better understanding of corneal cell biology to the table prior to surgery in order to produce optimized laser ablation profiles and less inflammation, especially in crosslinked corneas. If we can solve that problem, then we can make an already safe and successful procedure even safer, with even better outcomes.
1. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-A–induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620-627.
2. Kling S, Hafezi F. An algorithm to predict the biomechanical stiffening effect in corneal cross-linking. J Refract Surg. 2017;33:128-136.
3. Kling S, Hafezi F. Individualizing biomechanical stiffening in CXL. Cataract & Refractive Surgery Today Europe. 2018;5:32-33.
4. Chatzis N, Hafezi F. Progression of keratoconus and efficacy of pediatric [corrected] corneal collagen cross-linking in children and adolescents. J Refract Surg. 2012;28(11):753-758.
5. Panos GD, Kozeis N, Balidis M, Moschos MM, Hafezi F. Collagen cross- linking for paediatric keratoconus. Open Ophthalmol J. 2017;11:211-216.
6. Makdoumi K, Mortensen J, Crafoord S. Infectious keratitis treated with corneal crosslinking. Cornea. 2010;29:1353-1358.
7. Bunsen RW, Roscoe HE. Photochemical researches: Part V. On the measurement of the chemical action of direct and diffuse sunlight. Proceedings of the Royal Society of London. 1862;12:306-312.
8. Richoz O, Hammer A, Tabibian D, Gatzioufas Z, Hafezi F. The biomechanical effect of corneal collagen cross-linking (CXL) with riboflavin and UV-A is oxygen dependent. Transl Vis Sci Technol. 2013;2:6.
9. Knyazer B, Krakauer Y, Baumfeld Y, Lifshitz T, Kling S, Hafezi F. Accelerated corneal cross-linking with photoactivated chromophore for moderate therapy-resistant infectious keratitis. Cornea. 2018;37:528-531.
10. Richoz O, Kling S, Hoogewoud F, et al. Antibacterial efficacy of accelerated photoactivated chromophore for keratitis-corneal collagen cross-linking (PACK-CXL). J Refract Surg. 2014;30:850-854.
11. Hafezi F, Koller T, Derhartunian V, Seiler T. Pregnancy may trigger late onset of keratectasia after LASIK. J Refract Surg. 2012;28:242-243.
12. Gatzioufas Z, Panos GD, Tabibian D, Hafezi F. Ocular anterior segment changes and corneal biomechanics in pregnancy. J Cataract Refract Surg. 2015;41:480-481.
13. Tabibian D, de Tejada BM, Gatzioufas Z, et al. Pregnancy-induced changes in corneal biomechanics and topography are thyroid hormone related. Am J Ophthalmol. 2017;184:129-136.
14. Richoz O, Arba Mosquera S, Kling S, et al. Determination of the excimer laser ablation rate in previously cross-linked corneas. J Refract Surg. 2014;30:628-632.
15. Hafezi F, Gatzioufas Z, Angunawela R, Ittner LM. Absence of IL-6 prevents corneal wound healing after deep excimer laser ablation in vivo. Eye (Lond). 2018;32:156-157.
