



When ophthalmic surgeons plan for refractive surgery or premium IOL implantation, we evaluate the patient’s corneal topography, test for dry eye disease, and take extensive biometric measurements as a basis for calculating IOL power. We do not, however, achieve the same level of understanding regarding the visual demands of the patient’s lifestyle. Nor do we truly monitor the patient’s vision in the way that a glaucoma specialist monitors IOP or a cardiologist monitors systemic hypertension.
Our patients’ visual tasks and demands vary throughout the day, and often they do not have the observational skills or the language to communicate those demands to us. Wouldn’t it be helpful to monitor a patient’s visual performance and environment throughout the day in order to have an objective measure of their visual demands?
I recently gained experience with the Visual Behavior Monitor (VBM; Vivior), a device that can be clipped onto prescription or clear spectacles to record the patient’s daily activities for 3 to 5 days. The device contains sensors to measure distance, ambient light, head orientation, and motion. The data are then uploaded to the cloud for processing and analysis.
My experience has demonstrated to me that this technology can be used to improve refractive outcomes for cataract and refractive surgery patients. The information it records allows surgeons to understand the individual patient’s visual demands preoperatively and to postoperatively monitor how well his or her new vision meets those demands throughout the day.
PATIENTS DON’T KNOW THEIR NEEDS
Clinicians currently attempt to understand their patients’ visual demands through guesswork or by asking patients about their daily activities. Either of these methods, however, is subjective, and inaccurate information gathered in these ways can hinder one’s surgical success rate. Even patients themselves do not understand what kinds of distance vision they need for which periods during the day.
Physicians can measure a patient’s blood sugar by the hour, but it has seemed impossible to obtain similar types of real-time measurements for vision. We cannot measure the distance of vision tasks as our patients go about their day, whether in the office, driving home, playing golf, or cooking. Patients cannot spend the day holding a ruler in their hands to gather these measurements.
This lack of real-life, real-time data makes surgical planning challenging, especially for presbyopia-correcting surgery, such as the implantation of a multifocal IOL. Different professions and lifestyles may require different approaches. It is impossible for a surgeon to estimate, for example, the distance at which a chef does most of his or her cooking, or a mechanic does most of his or her repair work. The VBM helps solve this problem by allowing surgeons to obtain objective evaluations through real-time monitoring of their patients’ vision.
In premium cataract surgery, we are not only changing patients’ vision but also potentially affecting their lifestyle and quality of life. Providing a patient with the ability to read the smallest letters from the nearest distance without the need for spectacles might be considered a success for the surgeon. However, if we did not take into account the actual visual demands presented by the patient’s lifestyle and the patient’s expectations for meeting those demands, that result might be seen as a failure by the patient.
No two patients are exactly the same. The aforementioned hypothetical chef and mechanic, each coming in for surgery to fix their presbyopia, will need to be treated differently, as would a bus driver (see Case Report) or an attorney. In order to plan appropriately for each individual surgery, we need objective data from the patient, not subjective data based on asking patients about their daily professional and leisure activities.
This patient is a bus driver. As shown in Figure 1, he drives in the morning and afternoon, and he performs these duties mostly by looking at a far distance. Between noon and 1 pm, presumably during lunch, he has stable vision at a closer 1.5 m.
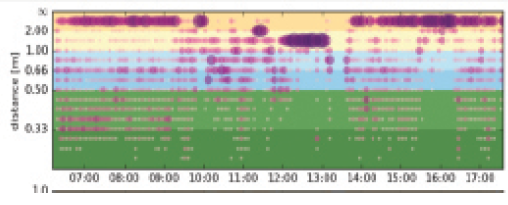
Figure 1. Purple represents the distance at which visual tasks are performed. The different colored bands indicate the distance at which most of the user’s attention is directed.
The color scale provided by the Visual Behavior Monitor (Figure 2) is another graphic representation of the patient’s visual demands. It shows that he mostly uses long-distance vision during the day.
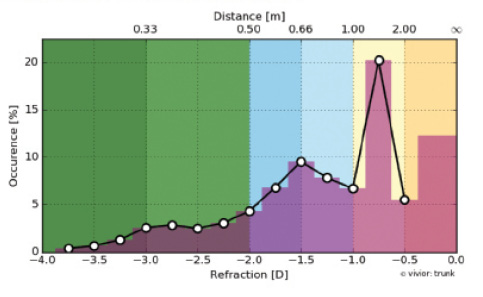
Figure 2. This graph shows the distribution of time spent at specific working distances. (Key: dark yellow, 2 m or more; yellow, 1–2 m; blue, between 50 cm and 1 m; green, 0–50 cm)
Figure 3 shows that the patient is in a bright environment while he drives but is indoors in dimmer light when he is not driving.
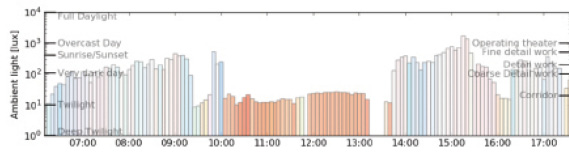
Figure 3. This graph shows the ambient light conditions at different times of the day.
INDISPENSABLE DATA
The data I can obtain from the VBM technology has become indispensable in our clinic for cataract and refractive surgery patients, especially those receiving premium IOLs. I would much rather plan for surgery by attaining an in-depth understanding of a patient’s lifestyle and visual demands through detailed measurements taken over several days than by evaluating visual acuity during a 5-minute exam.
The following is one example of how these data can be helpful. One of my patients who is an attorney was dissatisfied with her vision after presbyopia surgery. Even though she clearly explained to me that she had a desk job, I only realized after the surgery that she worked most of the day by reading at a book on her desk and then turning her head to her computer screen while she typed. If her vision had been monitored in her office for several days with the VBM, I would have realized that she was moving back and forth between two distances of vision: reading distance and computer distance. I could have planned her surgery differently and increased the patient’s satisfaction.
Since we have begun using the VBM device, our patients’ satisfaction with surgery has increased. Its ability to provide continuous monitoring and objective data on our patients’ visual demands has helped me provide better outcomes for my patients (see Advantages of Gathering Objective Data ).
ADVANTAGES OF GATHERING OBJECTIVE DATA
Provides continuous monitoring the patient’s visual demands.The evaluation of a patient’s vision through the measurement of visual acuity may not be sufficient to design a refractive surgery plan that has the potential to change the patient’s quality of life. Continuous monitoring of the patient’s vision for 3 to 5 days with the VBM provides a wealth of information to the surgeon.
Gathers objective data regarding the patient’s visual demands. Surgical plans for near or intermediate multifocal and trifocal IOLs, monovision LASIK, monofocal IOLs, and phakic IOLs are all created based on patients’ lifestyles and needs. Patients do not know how many centimeters of distance they need for various tasks during the day, nor is it easy for patients to communicate their visual demands. With the VBM, these objective data can be obtained.
Performs continuous monitoring of the brightness of the patient’s environment. The VBM shows how long the patient spends in bright and dark environments. This is another important factor in premium IOL performance that cannot be obtained reliably from patients because of its subjective nature: An objectively bright environment might be considered dark by the patient, and vice versa.
Improves the patient experience. The VBM helps communicate to patients that they are being offered customized care. Examination of the patient’s vision over 3 to 5 days increases the patient’s trust in the surgeon and helps improve the impression of the surgical experience.
Potentially improves the experience of dissatisfied IOL patients. The VBM can be used to show patients that surgery was planned correctly based on their presurgical measurements. It can also be used postoperatively to find out whether the patient’s visual demands have changed.
Offers user-friendly operation. The VBM is light and easy to use, and it does not touch the eye or the skin of the patient. The patient can remove the device whenever desired and then resume when ready.
