



Marfan syndrome was first diagnosed in 1896 by Antoine-Bernard Marfan as an inherited disorder of connective tissue. It is an autosomal dominant connective tissue disorder with cardiovascular, ocular, and skeletal abnormalities; 25% of individuals with Marfan syndrome have a spontaneous genetic mutation. This disorder affects approximately two to three out of 10,000 individuals, and more than 400 types of mutations have been observed.1
Marfan syndrome is caused by a mutation of the extracellular matrix protein fibrillin 1 (chromosome 15q21.1). Fibrillin is an important component of elastic fibers, and this genetic defect leads to an exuberant production of transforming growth factor beta. This change in fibrillin leads to a weakness of the connective tissues.2

The importance of recognizing Marfan syndrome
The diagnosis of Marfan syndrome relies on a set of formal criteria known as the Ghent nosology, a set of major and minor manifestations in multiple body systems.3 With improved treatments available and advances in diagnostic technologies for cardiovascular conditions, life expectancy and quality of life can be improved significantly for patients with Marfan syndrome. The phenotypic appearance of the disorder can differ widely in the severe form of neonatal Marfan syndrome, which leads to early death to patients who are otherwise healthy.
This is why every case of lens luxation should be considered a possible indicator for Marfan syndrome. Early diagnosis can help save lives, as the progression of an aneurysm can be treated early with beta-blocker or angiotensin-1-blocker therapy.

Ophthalmic Disorders With Marfan Syndrome
The effects that Marfan syndrome has on the eye can be divided into major and minor criteria. Ectopia lentis and lens coloboma of any degree are major criteria.3 At least two of the following minor criteria must be present in order to make a diagnosis: an abnormally flat cornea, increased axial length, and hypoplasia of the ciliary muscle or iris, causing decreased mydriasis.
Mean keratometry values of less than 42.00 D are highly correlated with a diagnosis of Marfan syndrome. Other secondary manifestations are early severe myopia, retinal detachment, early cataracts, glaucoma, amblyopia, and strabismus. Ectopia lentis occurs in 50% to 80% of patients with Marfan syndrome and is often the presenting sign of the disorder. Lens subluxation produces visual changes, primarily due to refractive errors such as high myopia, astigmatism, and induced anisometropia.

What Should Ophthalmologists Do?
Frequent observation of every patient with suspected Marfan syndrome is important. This is especially so in children because myopia and astigmatism caused by lens dislocation can lead to amblyopia. Photographic documentation of the grade of luxation (Figure 1), followup of the refractive error, and ocular wavefront analysis are important tools to analyze possible progression. Patients must be informed about all possible symptoms such as retinal detachment, glaucoma, and sudden lens dislocation into the vitreous.
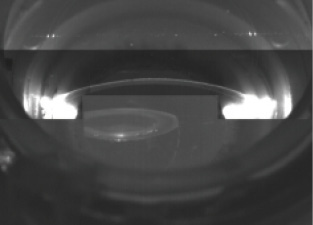
Figure 1. This scan showing a dislocated lens was helpful in reaching a diagnosis of Marfan syndrome.
Surgery to repair a dislocated lens is the most important treatment. Because of improved standards in care, early surgical intervention is recommended—even in children—if the patient’s refractive error is getting worse and lens ectopia or coloboma are increasing. The longer the surgeon waits, the more the risk of intraoperative complications rises and the option of saving the capsular bag becomes less likely.
Use of a femtosecond laser can make lens surgery more comfortable for the surgeon and safer for the patient. Achieving a nearly normal in-the-bag IOL implantation is possible in most cases of Marfan syndrome. However, if intraoperative complications occur, scleral fixation or iris-clip fixation of the IOL may be necessary.

Surgical Pearls
The capsulotomy is, without a doubt, the most difficult aspect of performing cataract surgery in patients with dislocated lenses. Manual capsulotomy causes additional stress on the zonula, which may lead to more intraoperative damage, and, if too severe, to a complete loss of the lens or the capsular bag.4 Vitrectomy is often necessary, which makes the operation even more complex.
In 2013, my colleagues and I performed the world’s first laser cataract surgery on a dislocated lens of a 23-year-old man with Marfan syndrome.5 We now perform laser cataract surgery in every dislocated lens in Marfan patients, if possible, with the capsulotomy diameter individualized for each patient and centered on the lens apex.

Surgical Technique
When a femtosecond laser is used in Marfan syndrome patients with ectopia lentis, the surgical technique includes the following key steps:
- Capsulotomy and lens fragmentation are performed with the femtosecond laser (Figure 2);
- Due to the typically young age of patients with Marfan syndrome, the fragmented lens can be aspirated without ultrasound energy. If necessary, the bag is stabilized with iris hooks enclaved into the capsulotomy;
- A 9-mm suture for the fixation of a capsular tension ring (CTR) is inserted with a long needle in the direction opposite from the ectopia and brought out of the eye with the help of a canula without damaging the capsular bag (Figure 3);
- The suture is fixated to the CTR, followed by implantation of the CTR in the capsular bag (Figure 4);
- When the knot is made in the suture, the capsular bag moves into a well-centered position; and
- A soft, hydrophilic, one-piece IOL is implanted through a 2.2-mm limbal incision into the capsular bag (Figure 5).

Figure 2. Manual capsulotomy in a patient with a dislocated lens.
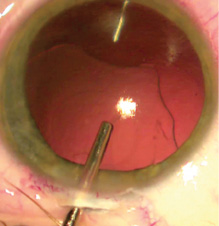
Figure 3. A 9-mm suture for fixation of a CTR is inserted in the direction opposite from the ectopia.
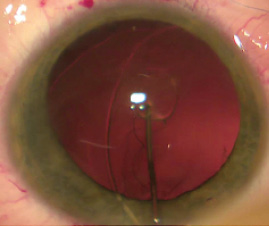
Figure 4. The CTR is implanted in the capsular bag.
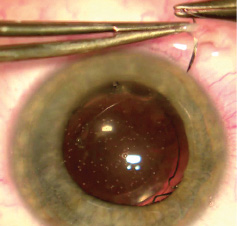
Figure 5. A soft, hydrophilic, one-piece IOL is implanted.
CONCLUSION
To date, our practice has used the technique described in Fundamental No. 5 in 12 eyes with dislocated IOLs. In all laser cataract surgery cases, the capsulotomy was performed without complications, and no intra- or postoperative adverse events have occurred. In all cases, visual acuity recovered quickly and refractive error (ie, lens-induced myopia and astigmatism) was decreased dramatically from preoperative levels. No late complications such as retinal detachment were observed.
After our positive experiences in these cases, the maker of our femtosecond laser, Lensar, established an extended scan mode in its software that allows additional scans, improving safety in the 3D reconstruction of the dislocated lens.
Laser-assisted capsulotomy of a dislocated lens is a very gentle and safe procedure. It offers the possibility of a standardized treatment option in these difficult cases. Positive results with this approach will lead to earlier treatment of ectopia in patients with Marfan syndrome and related disorders.
Because Marfan syndrome and its associated cardiovascular disorders can lead to sudden death, ophthalmologists have a responsibility to inform every patient with ectopia lentis about the effects of this syndrome and to begin an intense treatment regimen.
1. Maumenee IH. The eye in the Marfan syndrome. Trans Am Ophthalmol Soc. 1981;79:684-733.
2. Dietz HC, Cutting GR, Pyeritz RE, et al. Marfan syndrome caused by a recurrent de novo missense mutation in the fibrillin gene. Nature. 1991;352(6333):337-339.
3. Loeys BL, Dietz HC, Braverman AC, et al. The revised Ghent nosology for the Marfan syndrome. J Med Genet. 2010;47(7):476-485.
4. Anteby I, Isaac M, BenEzra D. Hereditary subluxated lenses: visual performances and long-term follow-up after surgery. Ophthalmology. 2003;110:1344-1348.
5. Holland, D. Surgical world premiere with Lensar femto laser at the Augenklinik Bellevue – Marfan surgery in dislocated lens. Electronic poster presented at: European Society for Cataract and Refractive Surgeons Winter Meeting; February 20-22, 2015; Istanbul, Turkey.



