


With the seemingly constant arrival of new IOLs that promise fewer visual disturbances and better outcomes designed for today’s visual requirements, we may one day look back fondly on the time when we focused more on patient selection than IOL selection to drive patient satisfaction.
Being familiar with all presbyopic IOL options and the type of visual benefits each offers is daunting enough. Then there is the added complexity of presenting the various options to your patients—particularly when those patients are not always the best at communicating their visual desires and needs.
But determining the best option is indeed an essential part of the customer service that patients expect when they walk through the door of your practice, and it’s what they will remember the longest. Yes, a warm welcome, a caring staff, and coffee are important, but what will have patients talking about your customer service long after surgery is how great their new vision is.
What if there were a way to objectively determine patients’ visual needs preoperatively, by gathering information about how they use their vision? The Visual Behavior Monitor (VBM, Vivior) promises to provide just such information.
PERCEPTIONS VERSUS REALITY
When clinical studies are conducted on presbyopic IOLs, study participants face a battery of tests, especially postoperatively, in order to assess visual acuity results, defocus curves, contrast sensitivity, and visual disturbances. By contrast, when patients are seen preoperatively in our practices, their visual acuity is measured, the necessary tests for IOL power calculation are performed, and the surgeon and his or her staff talks to them about how they use their vision and what their expectations are for their vision after surgery. There are few objective assessments like the ones that we apply after surgery to measure our results. Many of us use a visual assessment questionnaire to gather information about patients’ visual demands, but, again, these are subjective tools that rely on patients’ memories and expectations to guide our decisions.
At a time when the increasing sophistication of treatment options demands the use of more objective assessment methods, our reliance on patients’ recollection of how much time they spend reading or watching television has serious limitations.
OBJECTIVE EVIDENCE
In 2019, Vivior introduced the VBM, a wearable device designed to continuously monitor the user’s visual behavior. The VBM is fixed on the patient’s spectacle frame with a magnetic clip. (If the patient does not wear glasses, the VBM kit comes with a pair that can be worn.) Its sensors are capable of measuring distance to target, angle, gaze, and ambient lighting conditions. These data are downloaded onto a tablet, then uploaded to a cloud-based system where they are processed. The data can then be viewed via a web interface.
Surgeons receive a report that provides an objective picture of how much time the patient spends at each working distance for work and leisure activities, as well as the lighting levels under which the patient uses his or her vision.
PERSONAL TRIAL
The company has been conducting clinical studies to better understand how the VBM can be used in clinical practice. Ahead of participating in one of those clinical studies, one of us (GUA) tested the VBM by personally wearing the device, as well as getting several staff members to wear the VBM for 36 hours over a week’s time.
The objects of this effort were to understand personally what it is like to wear the device and to gather additional opinions from the staff. The experience revealed that the device was easy to use and not excessively obtrusive. It also yielded instructive data about how to provide a customized approach for each patient.
When we looked at the overall results from the 19 people who had worn the device both at work and at home, we found that the time spent on distance, intermediate, and near visual tasks was almost equally split, with an average of 33% of time spent at distance, 35% at intermediate, and 32% at near (see Professor Auffarth’s Personal Study).
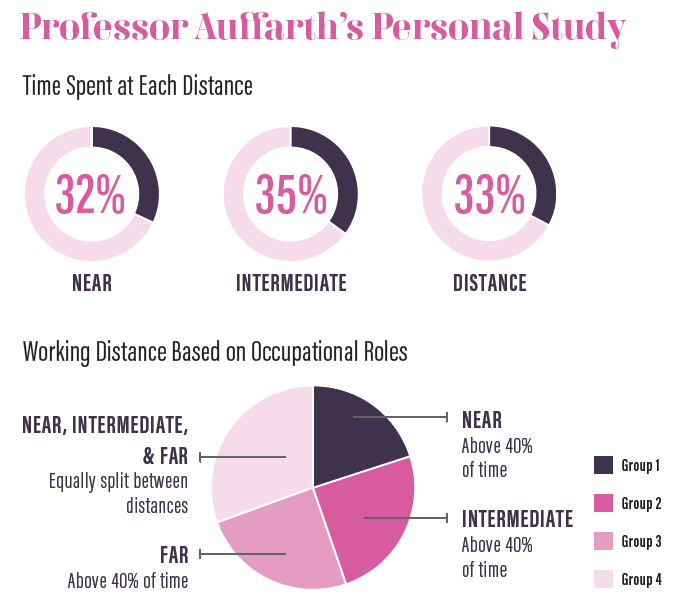
However, when we broke down the results based on the professional roles of each wearer, clear distinctions emerged. Among the administrative assistants and staff, the data showed that they spent 40% of their time working at near (group 1), whereas technicians and opticians spent a greater amount of time working at intermediate (group 2). A third group consisting of a variety of hospital professionals worked primarily at distance (group 3), and a fourth group—the surgeons (group 4)—spent their time moving equally among near, intermediate, and distance (see Professor Auffarth’s Personal Study).
Here we now had objective evidence that gave us a clear picture of how each individual used his or her vision. This exercise provided further evidence that patients really do require a customized approach to maximize their visual correction.
CHOOSING THE OPTIMAL IOL
At one time, we focused on patient selection when it came to presbyopic treatments. Today, we need to move on from this practice and adopt one in which we select the optimum IOL for the particular patient, based on objective information regarding how each patient uses his or her vision. We now have a tool, the VBM, to gather this type of information.
Adopting an objective approach could lead to better managing and matching of patient expectations. This should translate into a higher level of customer satisfaction with vision after presbyopia-correcting surgery, while also reducing the number of patients who are unhappy because their expectations were not met.
