


Cataract Surgery in an Eye With a History of Trauma and Floppy Eyelid Syndrome
Eric D. Donnenfeld, MD

A patient with a history of trauma and floppy eyelid syndrome presented for cataract surgery. Although the patient’s pupil was not very small, I decided to place an I-Ring pupil expansion device (Beaver-Visitec International) given the patient’s history of ocular trauma.
I use phenylephrine and ketorolac intraocular solution 1%/0.3% (Omidria, Omeros) for all of my patients whose insurance covers it, but especially if they have a history of ocular trauma, small pupils, intraoperative floppy iris syndrome (IFIS), or pseudoexfoliation. This strategy has dramatically reduced my need for pupil expansion devices.
surgical steps
Inserting the pupil expansion device. To begin the case, I inserted the I-Ring through a 2.2-mm incision to expand the pupil to 6.8 mm. I then positioned the device by adjusting its four positioning holes until the channels overlapped the iris, holding the pupil in place (Figure 1). The I-Ring offers many benefits during surgery; two that I particularly appreciate are that it doesn’t distort the iris and that it rarely causes iris sphincter tears compared with other pupil expansion devices. With the I-Ring inserted, I was able to perform the cataract surgery in a controlled manner.
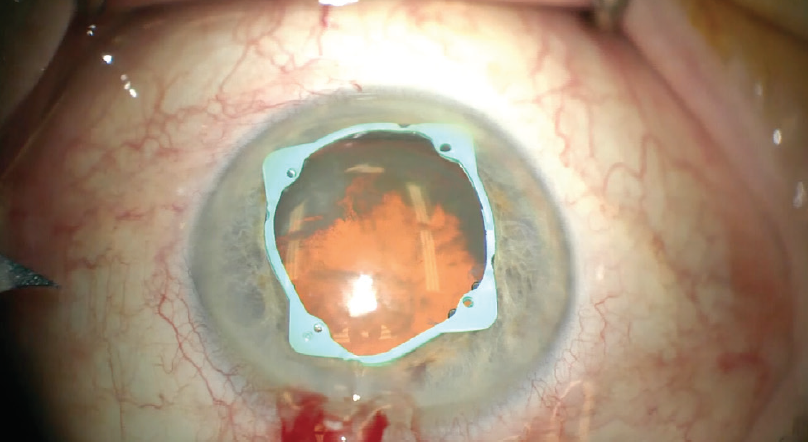
Figure 1. The I-Ring is placed by adjusting its four positioning holes until the channels overlap the iris to hold the pupil in place.
Capsulorhexis, phacoemulsification, and IOL insertion. I created the capsulorhexis and performed phacoemulsification using a slow-motion technique and low energy. I encountered a tear in the anterior capsule from previous trauma, so I inserted a three-piece IOL. I rotated the IOL into position and placed it in the sulcus.
Removing the expansion device. In my experience, removing the I-Ring is simple. The positioning holes are engaged in order to move the device inferiorly. It is frequently challenging to maneuver the device in the areas close to the wound, but the device’s soft material allowed easy manipulation in this case (Figure 2). All four positioning holes must be removed before the I-Ring can be disengaged from the eye. I used the insertion device to capture the I-Ring, close it, and pull it out through the incision.
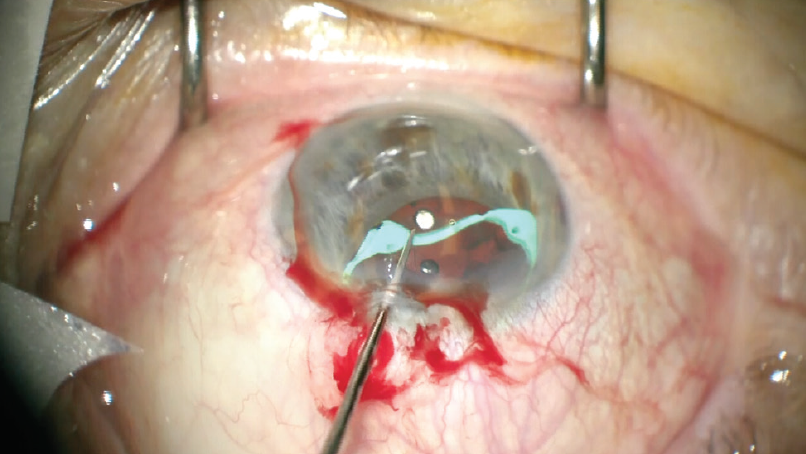
Figure 2. The I-Ring’s soft material allowed easy manipulation intraoperatively.
Figures 1 and 2 courtesy of Eric D. Donnenfeld, MD
Outcome
The patient’s postoperative recovery has been uneventful. The pupil is a normal size without distortion.
Poor Mydriasis and Compromised Zonules
Boris Malyugin, MD, PhD

Insufficient mydriasis is a difficult problem in cataract surgery that can be an indicator of various comorbidities. When a small pupil is associated with zonular pathology—as is often the case—surgeons face a particularly challenging situation with an increased risk of iris trauma, capsular rupture, vitreous loss, and inflammation.1 In these cases, surgeons must carefully evaluate multiple factors including pupil size, iris rigidity, sphincter fibrosis, and level of zonular weakness to determine their strategy.
In order to avoid complications, the pupil must be enlarged, and the lens capsule and zonular apparatus must be maintained. These goals can be achieved by use of a pharmacologic agent, incisional or stretching methods, or a pupillary expansion device. Instrument choice should be based on characteristics of the iris, such as floppiness or stiffness of the stroma or sphincter fibrosis. It is also vital not to challenge the integrity of the zonules by making the anterior chamber too shallow or overpressurizing the eye.
The following case description illustrates the importance of sound clinical judgement in determining the optimal technique and approach for a given patient with a small pupil and zonular pathology.
Presentation
A 79-year-old patient presented with cataract and pseudoexfoliation syndrome complicated by a small pupil and weak zonular support of the capsular bag. Even after the injection of a mydriatic agent, pupil dilation was not optimal. A pupil expansion device was therefore required to achieve better visualization.
Choosing the Expansion Device
My initial attempt at placing the 7-mm Malyugin Ring 2.0 (MicroSurgical Technology) was unsuccessful due to the rigidity of the patient’s pupil, which made it difficult to open the ring without also causing excessive stress to the iris tissue. Engaging all four scrolls of the ring proved challenging in this particular case, as the rigidity of the pupil and the flexibility of the device didn’t match. I therefore decided to remove the pupil expansion device and consider other options.
I decided to try the first-generation 6.25-mm Malyugin Ring Classic (MicroSurgical Technology) instead, which requires a slightly larger incision (2.2 mm) but offers the advantage of greater rigidity. This time, the rigidity of the device helped me manage the small, rigid pupil and achieve the dilation needed.
Managing Zonular Weakness
I was now facing a second difficulty: weak zonules. When zonular weakness is present, I like to start the capsulotomy using a sharp bent needle, which allows me to perforate the capsule with ease.
Because I had no support from the zonules, I needed a second instrument that could provide countertraction to stabilize the capsular bag while I performed the capsulorhexis. Therefore, I made a small capsular tear and placed one capsular retractor (Chang modification; MicroSurgical Technology); this enabled me to stabilize the capsular bag enough to complete the capsulotomy (Figure 3).
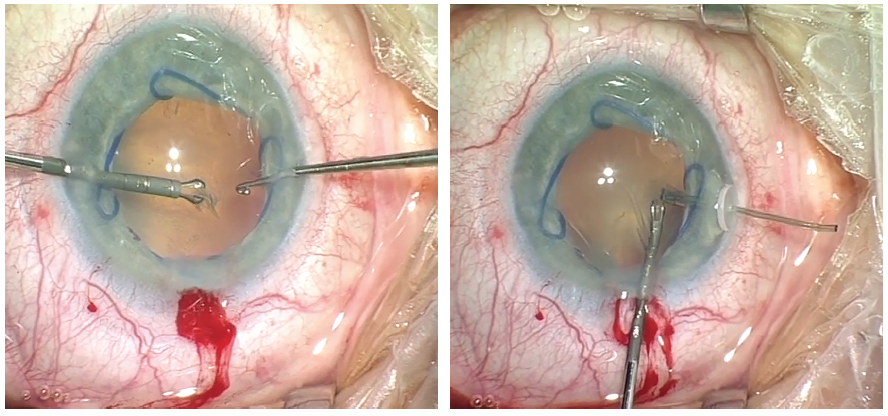
Figure 3. Continuous curvilinear capsulorhexis facilitated by the placement of capsular retractors is performed in a patient with weak zonular support.
To achieve support for phacoemulsification, I inserted three more capsular retractors. During phacoemulsification, I had to be cautious not to aspirate the capsular bag because the capsular equator in the spaces between the hooks was still unstable (Figure 4). Even though some residual cortical material was still present, I decided to insert a capsular tension ring to preserve the integrity of the capsular bag. With the capsular tension ring in place, I proceeded with cortical cleanup using a bimanual approach prior to IOL implantation.
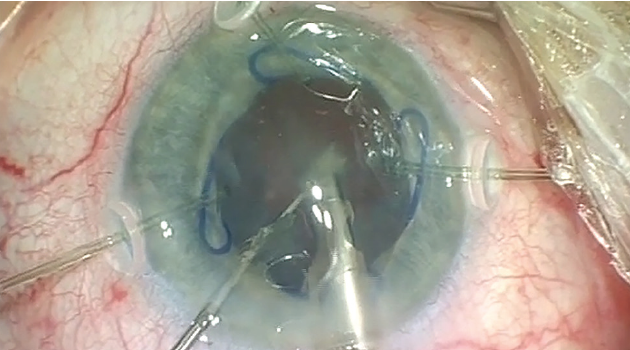
Figure 4. Phacoemulsification is performed with a Malyugin Ring and capsule retractors in situ.
Figures 3 and 4 courtesy of Boris Malyugin, MD, PhD
After removal of the capsular retractors, I implanted a three-piece IOL, which is my preference in these cases. Both haptic elements were inserted behind the iris into the ciliary sulcus, and the optic of the lens was prolapsed back through the capsulorhexis to achieve double support of the lens. Finally, I removed the pupil expansion device by catching the proximal scroll and retracting the ring.
Small Pupil Cataract Surgery Managed With an Iris Speculum
Cathleen M. McCabe, MD

We encounter small pupils in cataract surgery for a variety of reasons. Causes can include pseudoexfoliation, posterior synechia, the patient’s exposure to medications that induce intraoperative floppy iris syndrome, fibrotic membranes at the pupil margin, and intraocular manipulation or trauma to the iris.
When we are performing laser cataract surgery, a small pupil makes it difficult to create a properly sized capsulotomy with the laser. Toric IOL placement is also challenging if the pupil is small due to difficulty visualizing the orientation marks on the lens for proper positioning. The following case illustrates the management of a small pupil during cataract surgery and placement of a toric IOL.
Case Presentation
A 65-year-old man with a history of primary open-angle glaucoma presented with a nuclear sclerotic cataract and complaints of blurry vision and glare causing difficulty driving at night. His BCVA was 20/40 OU with a manifest refraction of +5.00 -0.75 x 065° OD and +5.00 -1.75 x 115° OS. Visual acuity decreased to 20/80 OD and 20/100 OS with glare testing. IOP was 16 mm Hg OD and 18 mm Hg OS with timolol b.i.d. OU. A visually significant nuclear sclerotic cataract was present in each eye. OCT imaging showed progressive thinning of the retinal nerve fiber layer in each eye with corresponding visual field defects on Humphrey visual field testing. After discussing the risks and benefits of various treatment approaches, we decided to proceed with cataract surgery with astigmatism correction and combined MIGS procedures in both eyes.
Surgical Procedure
A small pupil (< 4.2 mm) was noted in the right eye at the start of surgery despite repeated application of topical dilating medications (Figure 5). Ink dots were placed at the limbus using a cystotome needle, and the slit beam was oriented at the appropriate axis before the patient was taken to the femtosecond laser room, where corneal incisions were made and nuclear fragmentation was performed with the laser. I did not use the laser to create the capsulorhexis because the pupil was too small.
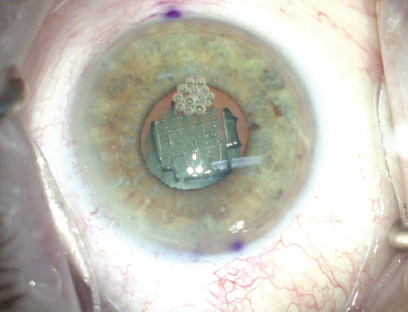
Figure 5. After femtosecond laser nuclear fragmentation, a small pupil (< 4.2 mm) is noted.
In the OR, an iris speculum (XpandNT, Diamatrix) was inserted into the anterior chamber (Figure 6) after the anterior chamber was filled with a dispersive OVD (Viscoat, Alcon). The four pockets of the flexible nitinol ring were positioned so that the edge of the pupil was gently cradled and stretched, enlarging the pupil diameter to 6.7 mm. If zonular laxity is present, this iris speculum device can also be used to capture the capsule edge and can act as a secure capsular support.

Figure 6. The XpandNT iris speculum pupil-expanding device enlarges the pupil diameter to 6.7 mm.
Phacoemulsification and removal of the cataract proceeded as in a normal case, with no movement of the iris and a safe and secure pupil margin, preventing trauma during phacoemulsification and cortical removal.
Visualization of the toric orientation marks was easy with the widely dilated pupil. After rotating the lens into place, the iris speculum was gently removed using the inserter, and 180° viscodilation of Schlemm canal and the collector channels was performed superiorly using the Omni Surgical System (Sight Sciences; Figure 7). A Hydrus Microstent (Ivantis; Figure 8) was then placed into Schlemm canal superiorly through the same incision through the trabecular meshwork.
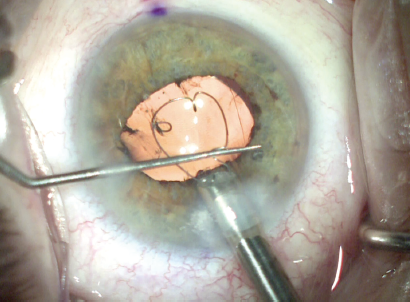
Figure 7. The iris speculum is removed using the inserter and viscodilation of the Sclemm canal and collector channels is performed using the Omni surgical system.
Figure 8. The Hydrus Microstent in place.
Figures 5-8 courtesy of Cathleen M. McCabe, MD
I have found that the combination of viscodilation using the Omni system and implantation of a Hydrus Microstent enhances the reduction of IOP. This finding also makes sense in theory, as the viscodilation opens Schlemm canal for a continuous 180° and expands the collector channels in that area. Once the Hydrus Microstent is in place, 90° of Schlemm canal is scaffolded open in an area that is, after viscodilation, now open for an additional 90°.
After removal of OVD from the anterior chamber, the pupil was round with no trauma or defects, and the toric IOL was aligned properly.
Postoperative Outcome
The second eye surgery was managed in a similar fashion. The patient’s postoperative distance BCVA is 20/25+2 OU with well-controlled IOPs without topical medication.
