



Presbyopia is an inevitable part of aging. Lens dysfunction that typically becomes symptomatic in our 40s progresses to visually significant cataract by our 60s. Treatment of presbyopia often begins with reading or bifocal glasses. Glasses are also commonly used after cataract surgery, but there are increasingly better surgical solutions involving presbyopia-correcting IOLs.
The decision of whether to choose a presbyopia-correcting IOL is often framed as one involving convenience, cost, and safety. Developed as an extension of refractive surgery, the correction of presbyopia at cataract surgery is treated by many eye care providers as a way of providing greater patient convenience. Consequently, many surgeons dislike dealing with the additional time and monetary costs—for both surgeon and patient—required to correct presbyopia during cataract surgery.
For surgeons, safety is a major consideration. The concept of “first, do no harm” drives our attitudes toward presbyopia correction. Unfortunately, many clinicians assume that glasses cause no harm and are therefore the safest default choice. On the other hand, the latest generation of presbyopia-correcting IOLs has a greatly improved risk-benefit ratio relative to earlier generations. That said, they are still presumed by many to carry higher risks—such as increased night vision symptoms and decreased visual quality—than glasses.
The literature suggests, however, that this presumption is inaccurate for patients with refractive error if one considers all the risks, both ocular and nonocular, of wearing multifocal glasses.1-4
POOR EDGE CONTRAST
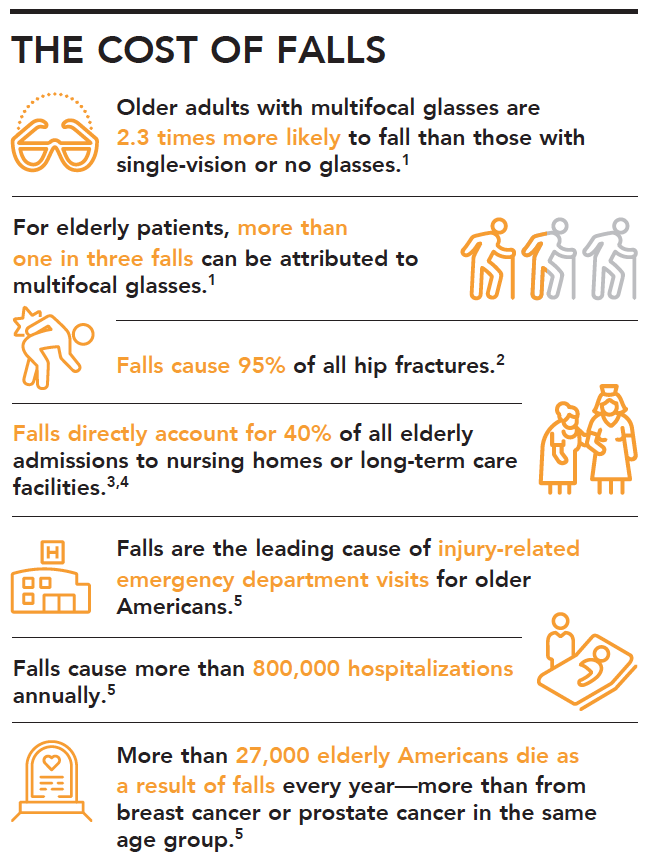
The add portion of multifocal (bifocal, trifocal, or progressive) glasses results in reduced edge-contrast sensitivity and depth perception for wearers, thus increasing the risks of tripping and falling, particularly on stairs.1 Older adults with multifocal spectacles are 2.3 times more likely to fall than those with single-vision or no glasses.1 Looking down at a step through the lower (near-add) portion of the lens, or viewing a target at an angle, so that each eye is looking through a different segment of the lens, can cause problems with depth perception and blur.
Poor edge contrast becomes particularly important when individuals venture outside their homes, where they may need to navigate different shades of carpet or flooring, uneven concrete, and unfamiliar obstacles. Additionally, prismatic jump at the top of the reading segment of a bifocal causes an apparent displacement of fixed objects.2 Studies, too, have found that multifocal spectacle wearers often misjudge vertical toe clearance when negotiating stairs, or they can miss the edge of a step.3,4
HEALTH CARE CONSEQUENCES
For elderly patients, more than one in three falls can be attributed to multifocal glasses.1 Ophthalmologists rarely see the health care consequences of these falls in our clinics, but they are significant for those affected and for the health care system overall. Consider these and the other statistics outlined in The Cost of Falls.
1. Lord SR, Dayhew J, Howland A. Multifocal glasses impair edge-contrast sensitivity and depth perception and increase the risk of falls in older people. J Am Geriatr Soc. 2002;50(11):1760-1766.
2. Parkkari J, Kannus P, Palvanen M, et al. Majority of hip fractures occur as a result of a fall and impact on the greater trochanter of the femur: a prospective controlled hip fracture study with 206 consecutive patients. Calcif Tissue Int. 1999;65:183-187.
3. Scott V, Pearce M, Pengelly C. Technical report: Hospitalizations due to falls among Canadians age 65 and over: An analysis of data from the discharge abstract database as presented in: Report on Seniors’ Falls in Canada (Section 2.2). www.phac-aspc.gc.ca/seniors-aines/alt-formats/pdf/publications/pro/injury-blessure/seniors_falls/technical-report-hospitalizations_e.pdf. Accessed January 27, 2020.
4. Falls facts and figures. Regional Geriatric Program of Eastern Ontario. www.rgpeo.com/media/57625/falls facts and figures oct 29.pdf. Accessed January 27, 2020.
5. Falls are leading cause of injury and death in older Americans [press release]. Centers for Disease Control and Prevention. September 22, 2016. www.cdc.gov/media/releases/2016/p0922-older-adult-falls.html. Accessed January 27, 2020.
Falls also threaten the independence and quality of life of seniors. Injuries sustained in a fall, or even the anxiety about falling again, can lead to a cascade of undesirable consequences, including depression, social isolation, functional decline, reduced quality of life, and greater likelihood of institutionalization.5,6
The cost to the health care system is also significant. In 2015, the total cost of all fall injuries to the US health care system was $50 billion, and that figure is expected to continue increasing.7 (By comparison, the entire US surgical ophthalmology industry accounts for about $6.3 billion annually.8)
PREVENTIVE STRATEGIES
Eye care interventions can reduce the risk of falls in the elderly. Simply performing cataract surgery, regardless of IOL type, can be quite beneficial. First-eye cataract surgery has been shown to reduce the fall rate by about 33%.9,10
The surgical correction of presbyopia at the time of cataract surgery can further reduce the risk of falls. Eliminating multifocal glasses has been shown to improve the safety of descending stairs11 and to reduce falls by up to 40% among people who regularly take part in outdoor activities.2
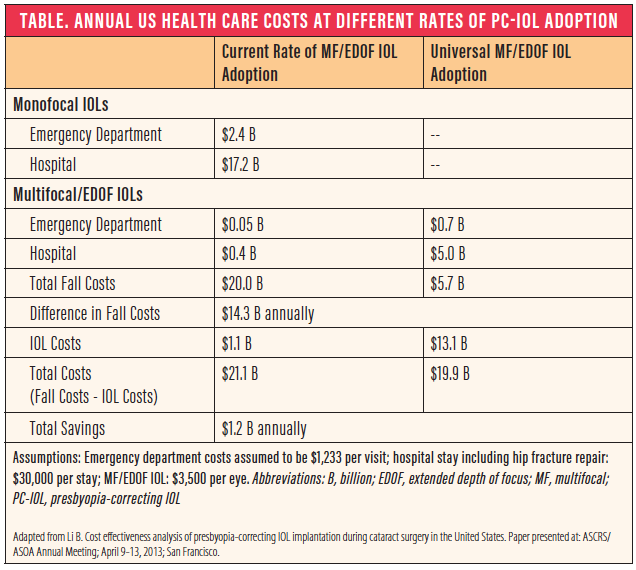
In a recent US cost-effectiveness analysis, Li compared the estimated costs for fall-related emergency department and hospital visits associated with bifocal spectacles given the current rate of presbyopia-correcting IOL adoption, to a hypothetical situation in which all patients receive a presbyopia-correcting IOL during cataract surgery.12 The savings in fall-related costs for emergency department and hospital visits was estimated to be more than $14 billion (Table). Even when the additional costs of the presbyopia-correcting IOLs were factored in, the savings to the health care system were still at least $1.2 billion, and the true savings are likely much higher because the analysis did not include costs for long-term care or other financial burdens borne by patients and their families.
RETHINKING RISK
Although provocative, this information does not imply that every patient should get a presbyopia-correcting IOL at the time of cataract surgery. Some patients are simply not candidates. Correction of refractive error at distance so that patients need only reading glasses and could thus be spectacle-free for safer ambulation is helpful. Providing separate prescriptions for distance and near single-vision glasses also helps to reduce the risk of falls.
Now that we know the risks associated with multifocal glasses, it is imperative that we broaden our definition and discussions of safety for older adults undergoing cataract surgery. When we take into account the reality of falls and injury, we must rethink what “do no harm” means in the context of cataract surgery and presbyopia correction.
Being wary of the potential visual quality and dysphotopsia issues of presbyopia-correcting IOLs is important, but it is arguably more important to factor in the risks of falls with bifocal glasses in the elderly. We should therefore give greater consideration to the surgical correction of presbyopia, which has the potential to prevent falls and to reduce the rate of injury, the loss of independence, and the risk of mortality in our older patients.
1. Lord SR, Dayhew J, Howland A. Multifocal glasses impair edge-contrast sensitivity and depth perception and increase the risk of falls in older people. J Am Geriatr Soc. 2002;50(11):1760-1766.
2. Haran MJ, Cameron ID, Ivers RQ, et al. Effect on falls of providing single lens distance vision glasses to multifocal glasses wearers: VISIBLE randomised controlled trial. BMJ. 2010;340:c2265.
3. Johnson L, Buckley JG, Scally AJ, Elliott DB. Multifocal spectacles increase variability in toe clearance and risk of tripping in the elderly. Invest Ophthalmol Vis Sci. 2007;48:1466-1471.
4. Davies JC, Kemp GJ, Stevens G, et al. Bifocal/varifocal spectacles, lighting and missed-step accidents. Safety Sci. 2001;38:211-226.
5. Masud T, Morris RO. Epidemiology of falls. Age Ageing. 2001;30(Suppl 4):3-7.
6. Peel NM. Epidemiology of falls in older age. Can J Aging. 2011;30:7-19.
7. Falls prevention facts. National Council on Aging. https://www.ncoa.org/news/resources-for-reporters/get-the-facts/falls-prevention-facts/. Accessed January 27, 2020.
8. Statista website. Value of U.S. ophthalmology market from 2009 to 2014 (in billion U.S. dollars). https://www.statista.com/statistics/445654/us-ophthalmology-market-size/. Accessed February 24, 2020.
9. Harwood RH, Ross AJ, Osborn F, et al. Falls and health status in elderly women following first eye cataract surgery: A randomized controlled trial. Br J Ophthalmol. 2005;89:53-59.
10. Palagyi A, Morlet N, McCluskey P, et al. Visual and refractive associations with falls after first-eye cataract surgery. J Cataract Refract Surg. 2017;43(10):1313-1321.
11. Timmis MA, Johnson L, Elliott DB, Buckley JG. Use of single-vision distance spectacles improves landing control during step descent in well-adapted multifocal lens-wearers. Invest Ophthalmol Vis Sci. 2010;51(8):3903-3908.
12. Li B. Cost effectiveness analysis of presbyopia-correcting IOL implantation during cataract surgery in the United States. Paper presented at: ASCRS ASOA Annual Meeting; April 9-13, 2013; San Francisco.
