
Ophthalmology marked a milestone on February 17, 2023, the day that the first complement inhibitor was approved for treatment of geographic atrophy (GA).
The approval of Syfovre (pegcetacoplan, Apellis) opens a new chapter as a first-in-class treatment. It was followed closely by avacincaptad pegol (Izervay, Iveric Bio), which gained the nod from the US FDA on August 5th, 2 weeks before its expected PDUFA date.
While it is too early to know what effect the introduction of complement therapy will have on GA moving forward, the approvals represent an important step ahead, according to retina expert Charles C. Wykoff, MD, PhD, who joined IJC for a virtual episode.
(Editor’s Note: This episode was filmed after the introduction of pegcetacoplan and before the approval of avacincaptad pegol).
“I believe GA has been one of the largest unmet needs in ophthalmology for the last 10 years, and we finally have a treatment for it. The treatment is a valuable, clinically meaningful step forward, but it has challenges, and we must continue to study them, learn from them, and eventually improve our therapeutics based on these learnings,” Dr. Wykoff said.
Some may be quick to compare this dawning era to the introduction of anti-VEGFs. However, with anti-VEGF therapy, response is often rapid, vision improves, and imaging changes over time. Those sorts of endpoints have not yet been established for GA.
“There were a lot of positive feedback loops with the anti-VEGF agents, with vision and anatomy both improving in most patients. It is a very different landscape with our current GA therapies which slow anatomic worsening but do not have a large, direct benefit on visual function within the time-frames or patient populations studied to date with these drugs,” Dr. Wykoff said.
What is Complement?
According to Dr. Wykoff, “the complement system is part of the innate immune system that is important for protecting our tissues from infectious diseases and also important for clearing damaged tissues. What we think may be happening at a simplistic level … is that maybe macular degeneration is being driven at least in part by an overactive complement cascade in the back of the eye in these sensitive tissues, causing slow accumulation of cell death over a lifetime of the patient.”
Thus, therapeutic inhibition is rational. To date, clinical trials have shown benefit in inhibiting C3, which is the common convergence point of the three known activating pathways (ie, pegcetacoplan), or C5 (ie, avacincaptad pegol), downstream from C3, but prior to the terminal pathway involving formation of membrane attack complex, the primary driver of cell death, including death of the retinal pigment epithelium (RPE).
Overall, results from both treatments appear comparable, though have never been directly compared in studies. How they are interpreted may be crucial to understanding their utility. On the one hand, each is associated with only modest improvements in reduction of geographic atrophy (Figure 2). 1-3 On the other hand, from the patient perspective, the potential to preserve vision means things like greater independence and better quality of life.
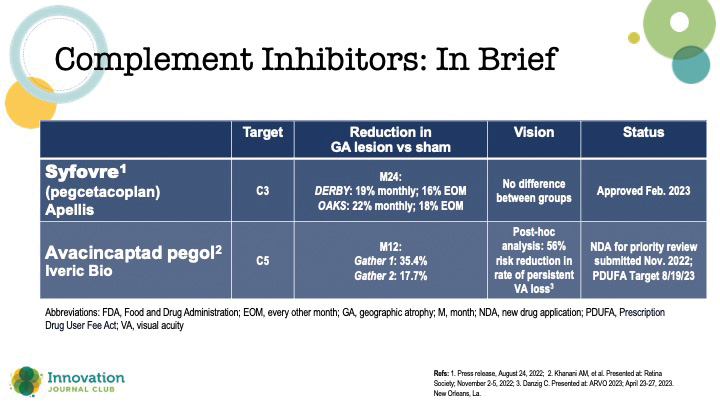
Figure 2. Comparison of complement inhibitors that have reached phase 3 or later.
As with any pharmaceutical product, safety must be discussed. Each medication has a unique profile, but some commonalities exist, including potential intraocular inflammation, ischemic optic neuropathy, and development of wet age-related macular degeneration (AMD). The latter raises an important point about monitoring for all ophthalmologists to be aware of if they have a patient undergoing complement inhibiting therapy.
“A key is to obtain consistent OCT imaging in patients who are receiving treatment to evaluate for early signs of exudation, which could be an indication of development of wet AMD. There are extensive data showing that the earlier wet AMD is diagnosed and the sooner patients receive appropriate treatment, the more likely patients are to achieve optimal outcomes,” Dr. Wykoff said. “We don't want to miss an early conversion to wet AMD in these patients.”
Additional Pearls
Readers of the phase 3 clinical trials for complement therapies will note frequent reference to fundus autofluorescence imaging (FAF). Although it is invaluable for measuring GA progression, FAF is infrequently and inconsistently used by ophthalmologists, “even retina specialists,” Dr. Wykoff said.
GA is characterized by death of the RPE, which appears on FAF as dark spots, or a hypoautofluorescent signal. When that spot is rimmed by a bright hue, a hyperautofluorescent signal, it means the atrophy is at risk of expansion, as the adjacent RPE cells are unhealthy.
While assessing risk for GA progression is well characterized with FAF, OCT b-scans are still the most commonly employed tool for making a diagnosis and managing patients with GA (en face may be helpful for mapping progression over time). Among the hallmark signs, hypertransmission, or passage of signal through the choroid, may be one of the most distinctive.
“There's increased signal in the choroid from the OCT because there is less attenuation by the photoreceptors and the RPE. If you see a bright signal in the choroid, which you normally don't, normally the choroid is slightly dark and shadowy … that’s a signal that there may be overlying areas of atrophy,” Dr. Wykoff said, adding that other diagnostic clues exist including sharp linear lines interspersed with darkened areas (potentially referred to as a barcode sign).
1. Apellis. Press release, August 24, 2022.
2. Khanani AM, et al. Presented at: Retina Society; November 2-5, 2022.
3. Danzig C. Presented at: ARVO 2023; April 23-27, 2023. New Orleans, La.

