


A patient presented with a visually significant cataract and dense congenital superior vascular and fibrotic posterior synechiae. Careful preoperative planning on how best to remove the cataract was required (Figure 1).
Figure 1. Cataract in an eye with a superior band of posterior synechiae, a prominent blood vessel, and a dense capsular opacity.
Surgical Approach
Manual cataract surgery with a temporal incision and staining of the anterior capsule was planned. The synechiae were left intact during the capsulotomy and cataract removal. An eccentric and oval capsulotomy was made. A chopper was used to retract the capsule to facilitate access by the phaco tip (Figure 2). A capsular tension ring was placed for support—the eyelets were oriented away from the capsular fornix under the area of adhesion because of the potential for a zonular defect in this area.

Figure 2. A chopper is used to retract the capsule and facilitate phacoemulsification.
The anterior capsule was polished to decrease fibrosis and phimosis (Figure 3). After the placement of a three-piece IOL in the capsular bag, microscissors were used to sever the central portion of the anterior capsular adhesion, free the pupil, and retract the iris so that the capsular scar could be inspected (Figure 4). Intraocular preservative-free phenylephrine was used to limit hemorrhaging when the vascular synechial band was cut with microscissors. The capsular opacity was left intact and dissected postoperatively using an Nd:YAG laser.
Figure 3. An anterior capsular polisher is used to decrease fibrosis.
Figure 4. Microscissors are used to sever the vascular adhesions.
Final pupil size was normal with an excellent surgical result (Figure 5).
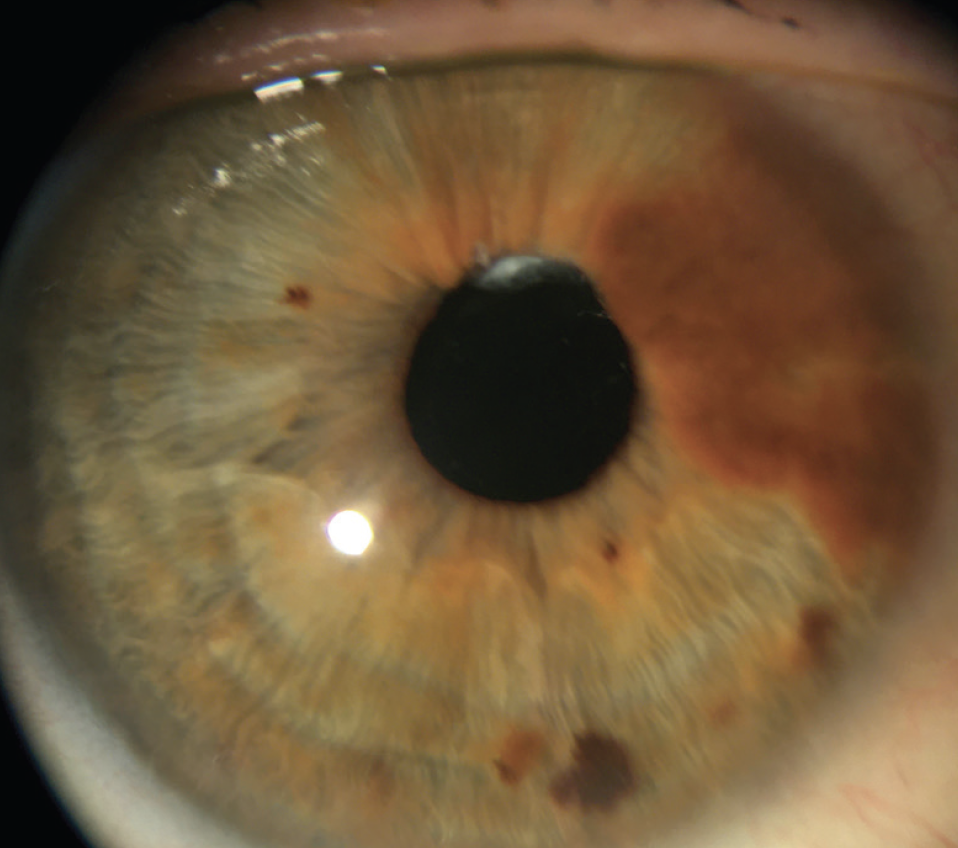
Figure 5. Postoperative photograph showing an excellent surgical result with a normal pupil size.



