


In the past, corneal graft procedures were performed infrequently at only a few ophthalmology centers worldwide. Today, however, more than 180,000 corneal grafts are performed each year.1 The change is due not as much to an increased need for corneal graft surgery as to a better understanding of the procedure’s benefits, more opportunities for skills transfer, and improved access to donor tissue. Moreover, new posterior and anterior corneal lamellar techniques have emerged and improved outcomes.2 Corneal graft failure remains a concern nonetheless.3,4
The main causes of corneal graft failure can be classified according to the mechanisms of failure.5 These are primary graft failure; immunological allograph rejection (early or late); and graft failure due to comorbidities such as glaucoma, ocular surface disease (OSD; eg, infectious keratitis and herpetic disease), corneal wound problems, and trauma. Corneal graft procedures are most likely to fail in pediatric patients. The main reasons for rejection in children are immunologic, followed by late endothelial failure and OSD. In adults, the main reason for rejection is glaucoma, followed by wound problems. Lamellar anterior keratoplasty has the lowest rate of midterm failure.
RESULTS OF A MULTICENTER STUDY
In a multicenter retrospective study conducted in Spain, the three main causes of graft failure were immunologic rejection, primary graft failure, and late endothelial failure (Figure).6 This study enrolled a consecutive cohort of 2,143 patients who underwent keratoplasty between 2001 and 2016 and were available for 1 year of follow-up. This is the largest cohort of patients analyzed in a single country in Southern Europe.
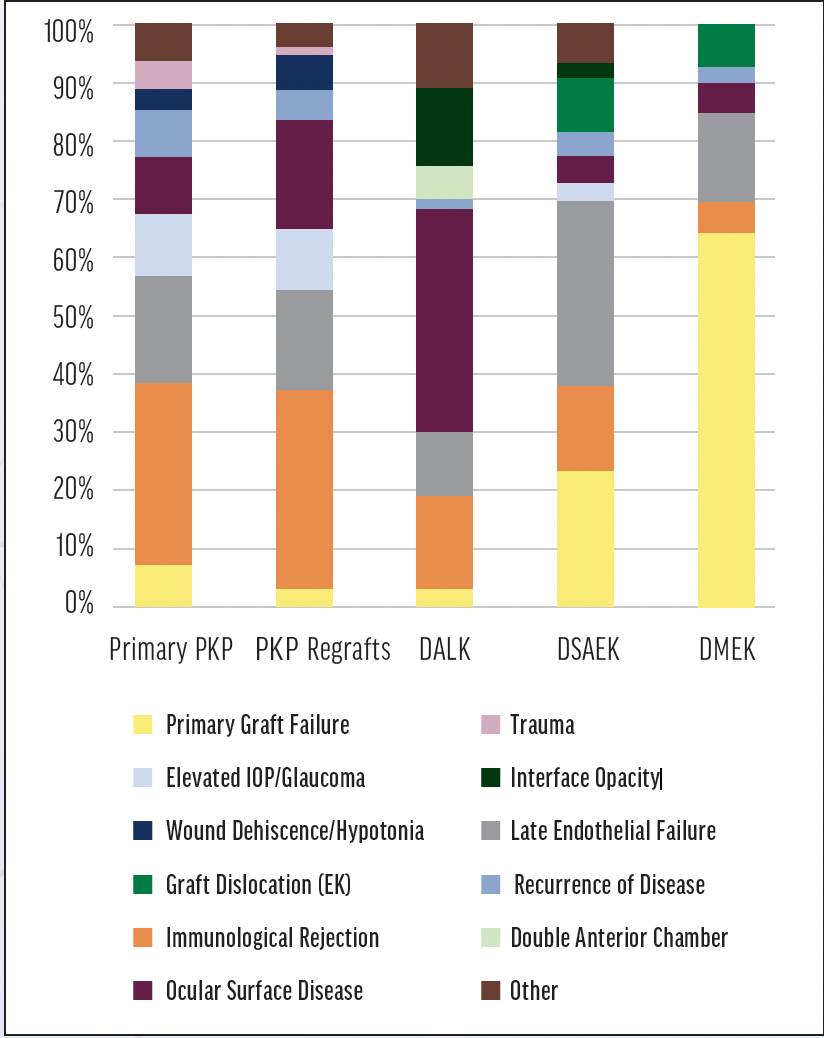
Figure. Causes of graft failure. Abbreviations: DALK, deep anterior lamellar keratoplasty; DMEK, Descemet membrane endothelial keratoplasty; DSAEK, Descemet stripping automated endothelial keratoplasty; EK, endothelial keratoplasty; PKP, penetrating keratoplasty
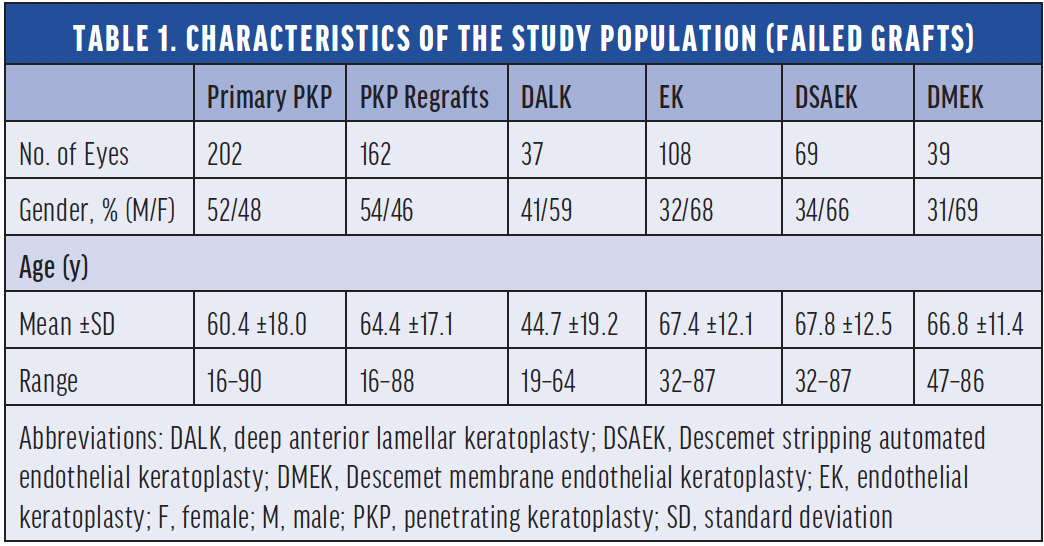
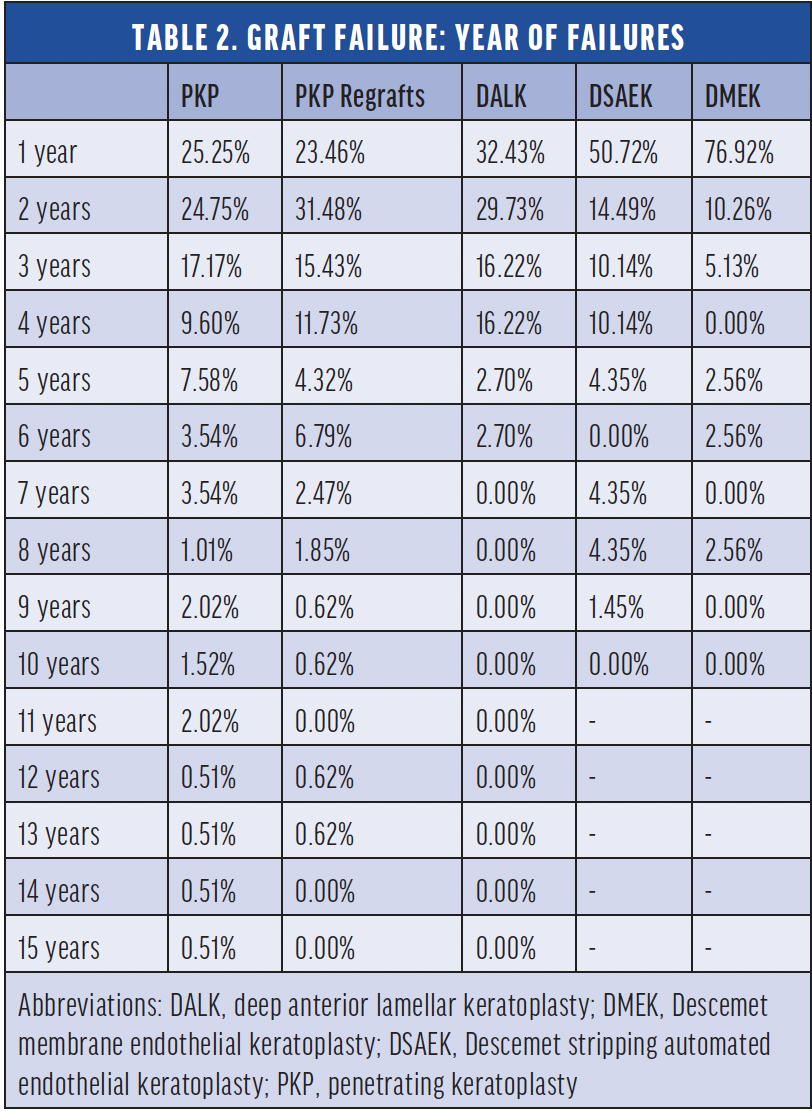
Graft failure, defined as the irreversible loss of graft transparency causing limited vision, occurred in 571 eyes. Immunologic allograph rejection was responsible for 28.2%, 34%, 16.2%, 14.5%, and 5.1% of the failures that occurred after primary penetrating keratoplasty (PKP), PKP regrafts, deep anterior lamellar keratoplasty (DALK), Descemet stripping automated endothelial lamellar keratoplasty (DSAEK), and Descemet membrane endothelial keratoplasty (DMEK), respectively. Primary graft failure was caused by OSD in 17.8% of cases and by late endothelial failure in 17.3%. The median time to failure for each graft type are shown in Tables 1 and 2, demonstrating that most endothelial keratoplasty grafts fail within the first year. This study confirms earlier reports that repeated keratoplasty is more likely to fail than primary PKP.7
Another common cause of graft failure after PKP and DSAEK was IOP elevation, emphasizing the importance of IOP control after corneal graft procedures. No association between elevated IOP and graft failure was found in the DALK or DMEK groups. Possible reasons are that corticosteroid use is lower in DALK and DMEK than in other keratoplasty procedures and that PKP is usually performed on eyes with more complex disease.
Results were also analyzed by the type of keratoplasty procedure. Graft failure after DALK occurred in 37.8% of cases. This was largely attributable to limbal insufficiency, keratolysis, or a persistent epithelial defect caused by OSD. Graft failure after DSAEK most often resulted from endothelial decompensation without rejection (31.9%), whereas the most frequent cause after DMEK was primary graft failure (64.1%).
The median time to graft failure varied by procedure type. Failure occurred within a median of 17.9 months after primary PKP, 11.6 months after DALK, and 7.8 months after DSAEK and DMEK. When primary graft failure was excluded, the median time to failure increased to 17.8 months for the DMEK and DSAEK groups. Most (77%) of DMEK failures occurred within the first year after the surgery.
In our experience, the main causes of graft failure are as follows: immunologic rejection for PKP, OSD for DALK, and primary graft failure for DSAEK and DMEK.8 We prefer endothelial keratoplasty (ideally DMEK) to PKP because we find that the former procedure is associated with faster visual recovery, a better postoperative refractive outcome, and greater refractive stability. The learning curve for endothelial keratoplasty procedures, however, is steep. Greater access to skills transfer opportunities could reduce the time required to master these techniques.
CONCLUSION
Our understanding and management of corneal graft failure is evolving. Efforts to address specific immunologic aspects of graft failure and incorporate the treatment of ocular surface inflammation into the surgical course are crucial.
Research on local and general immune suppression, improving ocular surface homeostasis, and immunologic management with advanced stem cell therapy is needed. Alternative surgical approaches using corneal organoids and tissue that are not at risk of immunologic allograph rejection could usher in a new era in the surgical treatment of corneal blindness.
1. Gain P, Jullienne R, He Z, et al. Global survey of corneal transplantation and eye banking. JAMA Ophthalmol. 2016;134:167-173.
2. Baydoun L, Muller T, Lavy I, et al. Ten-year clinical outcome of the first patient undergoing Descemet membrane endothelial keratoplasty. Cornea. 2017;36:379-381.
3. Price MO, Thompson RWJ, Price FWJ. Risk factors for various causes of failure in initial corneal grafts. Arch Ophthalmol. 2003;121:1087-1092.
4. Williams KA, Lowe M, Bartlett C, Kelly T-L, Coster DJ; Australian Corneal Graft Registry. Risk factors for human corneal graft failure within the Australian corneal graft registry. Transplantation. 2008;86:1720-1724.
5. Alio JL, Montesel A, El Sayyad F, Barraquer RI, Arnalich-Montiel F, Alio Del Barrio JL. Corneal graft failure: an update. Br J Ophthalmol. 2021;105(8):1049-1058.
6. Gómez-Benlloch A, Montesel A, Pareja-Aricò L, et al. Causes of corneal transplant failure: a multicentric ctudy. Acta Ophthalmologica. 2021;99(6):e922-e928.
7. Alió Del Barrio JL, Bhogal M, Ang M, et al. Corneal transplantation after failed grafts: options and outcomes. Surv Ophthalmol. 2021;66(1):20-40.
8. Montesel A, Alió Del Barrio JL, Yébana Rubio P, Alió JL. Corneal graft surgery: a monocentric long-term analysis. Eur J Ophthalmol. 2021;31(4):1700-1708.
