


We have had a long road of success with the Visian ICL (STAAR Surgical). Starting our journey with this lens in 2002, we have continued to increase our surgical volume year over year, and this has paralleled many refinements in the procedure and in the technology itself. The latest models, the EVO and EVO+ Visian ICL, have a hole in the center of the optic, which has eliminated the need to perform a peripheral iridotomy. The addition of this KS-AquaPort* has been a tremendous boost in the efficiency of the procedure. In this article, I discuss the medium- and long-term follow-up with this lens and review the clinical efficacy, predictability, and safety.
BACKGROUND
At the Instituto Universitario Fernández-Vega, we offer patients several forms of refractive surgical correction, including clear lens extraction with multifocal and monofocal IOLs, PRK, femtosecond LASIK, and implantation of the EVO family of Visian ICLs. In our experience, it is best to tailor the procedure to the individual needs of our patients, which, in many cases, ends up being the EVO Visian ICL. We have found that the sweet spot for the EVO Visian ICL can include patients under the age of 50 years with refractions ranging from 5.00 to -20.00 D. The key to ensuring safety with the procedure comes down mainly to three components: patient selection, selection of the proper ICL size, and lens vault evaluation and management.
Patient selection. The patient’s ocular anatomy must safely support a phakic IOL. In short, the rules of thumb that we use include the following:
- Anterior chamber depth 3 mm or greater;
- Iridocorneal angle above grade 3;
- Crystalline lens rise below 500 µm;
- Angle-to-angle greater than 11 mm; and
- Pupillary diameter greater than 9 mm.
ICL size selection. Once an eye is deemed safe for phakic IOL implantation, the next step is to select the proper size of the implant. In our practice, this should be equivalent to the following: ICL size = OCT horizontal angle-to-angle +1.0 mm. In case of doubt, the larger the white-to-white, anterior chamber depth, or crystalline lens rise, the larger the ICL size.
Lens vault evaluation and management. When implanting the phakic IOL, follow these general rules: the larger the ICL size, the greater the vault and the larger the ICL power, the greater the vault.
STUDY DESIGN
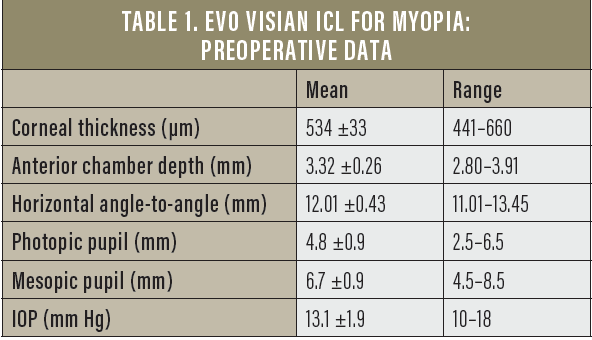
In 2017, we decided to review data from 186 myopic eyes that received the EVO Visian ICL at our practice and had at least 3 years’ follow-up. In total, 93 patients (63 women and 30 men) with a mean age of 30.4 ±5.4 years (range, 20†–45 years) were included in the study. Preoperative data can be found in Table 1.
Using the safety criteria described above, we selected the size of the EVO Visian ICL according to the OCT horizontal angle-to-angle measurements in each eye. In the majority of eyes (69.35%), a 13.2-mm EVO Visian ICL was implanted (Figure 1). Regardless of ICL size, we used the following surgical protocol:
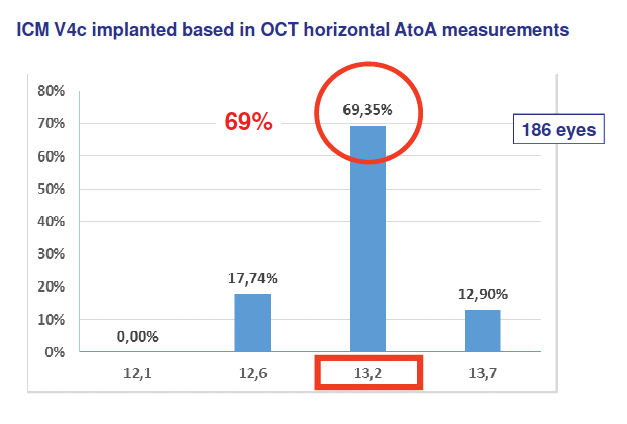
Figure 1. Sizes of the EVO Visian ICL implanted in the study.
- Day 1: Surgery on the first eye;
- Day 2: OCT of the first eye;
- Day 3: OCT of the first eye and surgery on the second eye;
- Day 4: OCT of the second eye; and
- Day 5: Standard exploration OCT of both eyes and database update by the optometrist.
RESULTS
Safety and efficacy. The safety and efficacy data, through 3 years of follow-up, can be found in Table 2. In short, the efficacy of the procedure ranged from 0.98 at 1 month postoperative to 0.89 at 3 years postoperative, and the safety remained consistent at 1.02 at 1 and 3 months and 2 and 3 years postoperatively. At 1 year postoperative, it was 1.03. This medium- and long-term follow-up confirms the safety and efficacy of the procedure.
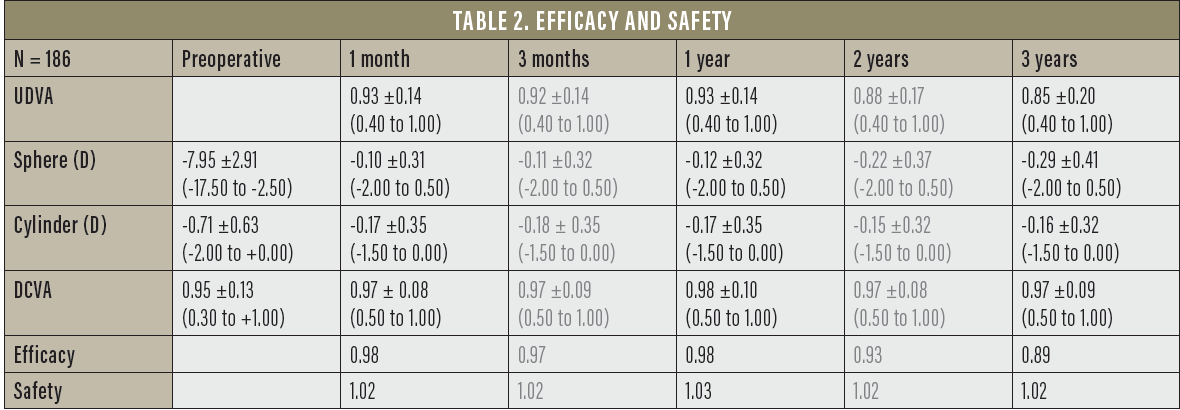
Predictability. EVO Visian ICL implantation is also a predictable procedure, and our results supported this. At 1 month postoperative, 97.2% of patients were within ±0.50 D of intended correction and 99.4% were within ±1.00 D. At 1 and 3 years, 95.6% and 80.6% of patients, respectively, were within ±0.50 D of intended correction and 99.4% and 95.6%, respectively, within ±1.00 D.
Evolution of vault. Vault also remained relatively consistent through 3 years postoperative (Figure 2). At 1 month postoperative, the mean vault was 478 ±204 µm (range, 90–1,080 µm), with only 8% of eyes outside the recommended range. At 1 and 3 years, the mean vault was 411 ±193 µm (range, 60–990 µm) and 350 ±164 µm (range, 40–960 µm), respectively, with only 10% and 6% of eyes, respectively, outside the recommended range.
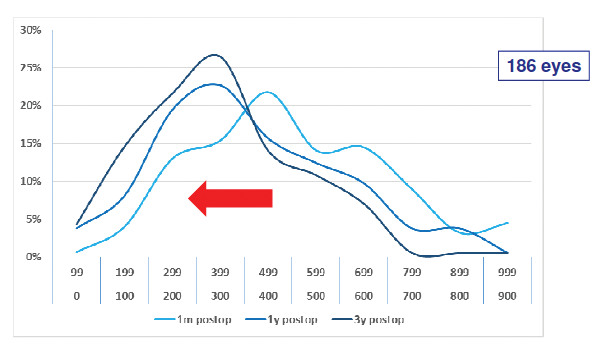
Figure 2. Evolution of vault from 1 month to 3 years postoperative.
What is also impressive about our study results was that there was no incidence of anterior subcapsular cataract postoperatively. In fact, this extends well beyond the study data. Since we began implanting the EVO Visian ICL—the model with the KS-AquaPort—in 2011, we have had zero anterior subcapsular cataracts in the 1,957 eyes we have treated with this procedure. Prior to this time, with a previous generation of the lens, we had experienced anterior subcapsular cataract formation postoperatively in 21 of 1,531 eyes, for an incidence of 1.37%. When this number (21) is taken into context with the total number of ICLs we have implanted (4,596), the incidence of cataract formation is a mere 0.46%. Again, each and every case of cataract formation occurred with a previous generation of the Visian ICL.
IOP. We also looked at IOP over time and found that all eyes had a good tolerance to high vault (Figure 3). This, again, is likely related to the addition of the KS-AquaPort, as it restores a more natural flow of aqueous humor within the eye.
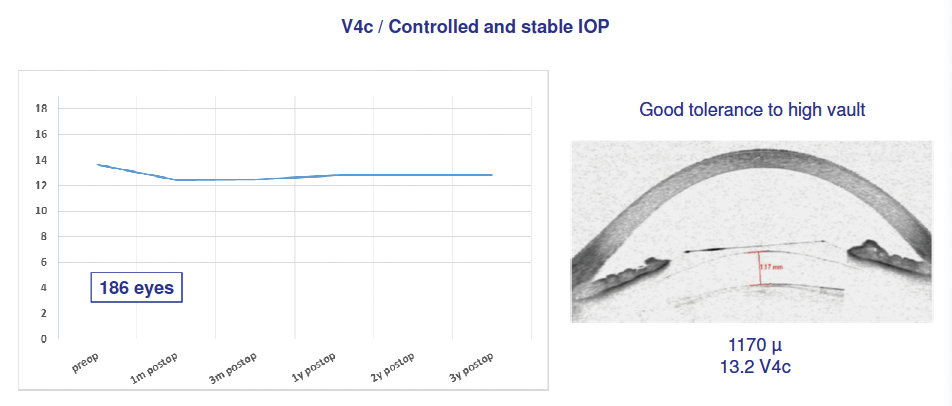
Figure 3. Eyes had a good tolerance to high vault, with controlled and stable IOP.
Endothelial cell loss. Our results also indicated that the amount of endothelial cell loss was controlled and stable across 3 years postoperative, from 2,700.39 cells/mm2 at 1 month postoperative to 2,661.07 cells/mm2 at 3 years postoperative.
CONCLUSION
In summary, our results have indicated that, with the correct vault of the EVO Visian ICL and the addition of the KS-AquaPort, the risk for cataract formation postoperatively is nearly eliminated. In order to ensure that the optimum vault is reached, we have found it useful to incorporate OCT with the Rescan 700 (Carl Zeiss Meditec).
When vault is low, we wait and monitor (Figure 4A), and when the vault is high, we rotate the EVO Visian ICL into a different position (Figure 4B). Our safety protocol is described in Figure 5.
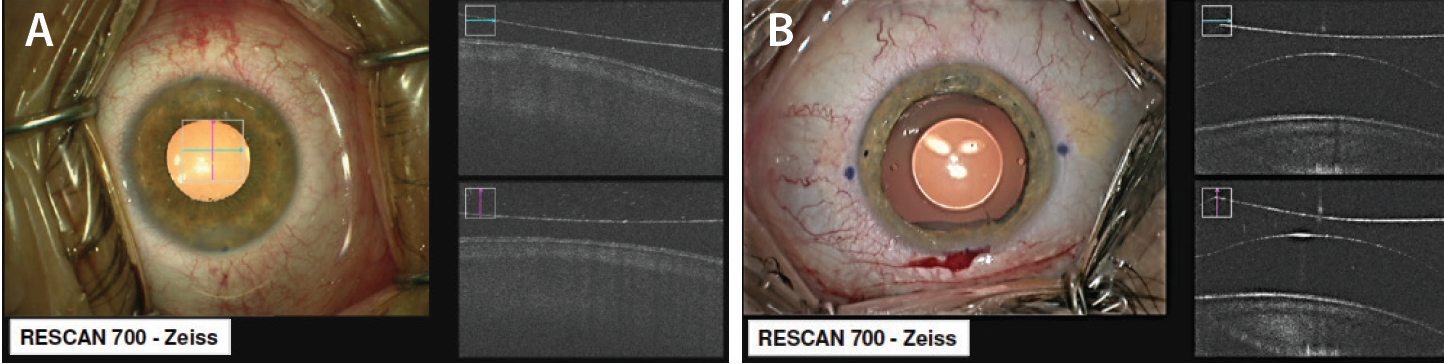
Figure 4. Intraoperative OCT.
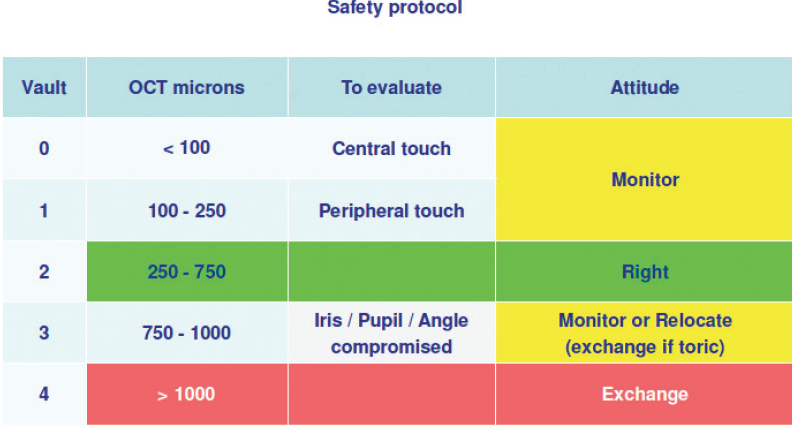
Figure 5. Safety protocol with the EVO Visian ICL.

