
I have been performing refractive surgery now for many, many years. When it comes to deciding what procedure is right for my patients, I consider all of the options that we have and select what I feel is the most ideal solution. In my experience, what makes the EVO Visian ICL (STAAR Surgical) the ideal refractive surgery procedure in so many cases is its efficacy, predictability, removability, and safety and its potential to help patients achieve excellent visual results postoperatively, including gained lines of distance BCVA. Implanting a phakic IOL like the EVO Visian ICL also accommodates patients’ future needs and allows the best outcome both immediately and down the line when the patient requires cataract surgery.
In the past, I tended to use the EVO Visian ICL mainly in eyes with high myopia and in some cases moderate myopia. Now, given recent data, I have expanded my recommendations with this lens to include eyes with low myopia as well. Given all of the properties of the EVO Visian ICL that make it an ideal solution for refractive correction, I am quite pleased to be able to offer this option to a wider range of patients.
A JOURNEY BACK
The evolution of the Visian ICL has been exciting, and with the latest EVO model, the company has now eliminated all of the barriers that have previously been raised about the use of phakic IOLs for refractive correction (Table 1) for my practice in Saudi Arabia.
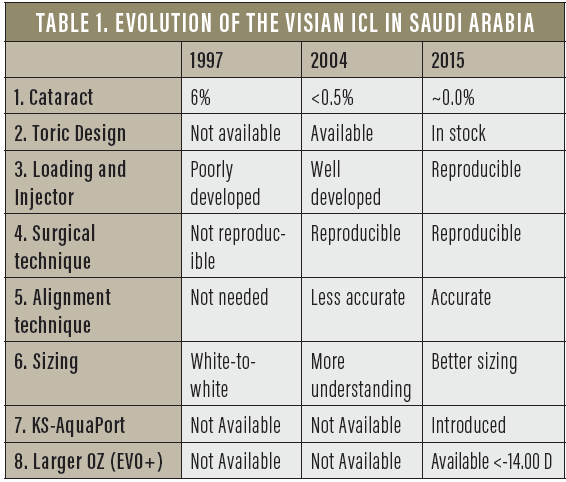
Anterior subcapsular cataract. Even though the rate of anterior subcapsular cataract has always been relatively low (for example, in my experience 6.6% before 1997 and 0.5% between 2005 and 2015), it is now eliminated completely with the addition of the KS-AquaPort, a small hole in the center of the optic that helps to return the flow of aqueous humor to a more natural state (Figure 1). Since I have been using this version of the lens in 2015, I have not had one eye develop an anterior subcapsular cataract.
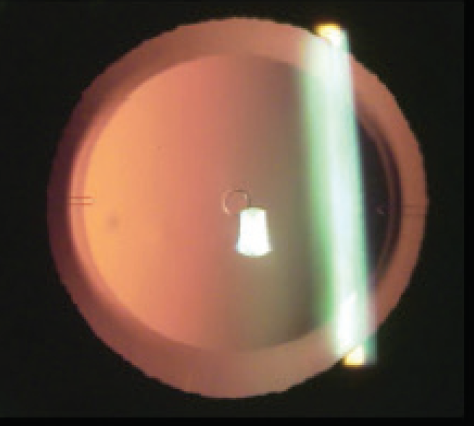
Figure 1. No incidence of cataract formation with the EVO Visian ICL.
Sizing. Another area of concern for some has been selecting the adequate size of the lens. (Editor’s note: This topic is covered in the article beginning on page 10 of this educational material. EVO Visian ICL: 10 Years of Follow-Up) But with each evolution of design, sizing has become increasingly easier.
Over the past decade, we compared many techniques for ICL sizing using different technologies including white-to-white (WTW) horizontal diamter, sulcus measurement with high-frequency ultrasound, and angle-to-angle diameter using anterior segment OCT. We concluded that using the WTW diameter is good enough in more than 95% of the cases. Using WTW diameter, our rate of ICL exchange due to improper sizing in the last 3 years was 1%.
Optic size. With the introduction of the EVO+ Visian ICL, we are now able to better accommodate the ocular anatomy of patients with larger pupils. The latest model, the EVO+, has an expanded optical diameter up to 6.1 mm depending on lens power, which improves the quality of vision especially at mesopic conditions. With the the EVO Visian ICL design, the functional optical zone is larger than previous designs and is much larger than any laser vision correction procedure; this makes the superiority in quality of vision more significant when compared to laser procedures.
PATIENT OPTIONS
Now the EVO Visian ICL can be recommended for use in a wider range of patients. This is in part due to the updated design, which can accommodate patients with larger pupils, and also in part due to the fact that it can effectively treat lower amounts of myopia and astigmatism than previously attempted. We can also use the EVO Visian ICL across a wider age range, and bilateral surgery has become a routine practice.
Today I often use the lens in eyes that are good candidates for LASIK because I believe in the procedure, and I know that it truly offers my patients the closest to ideal refractive correction.
My colleagues and I recently performed a retrospective anaylsis of the EVO Visian ICL for the treatment of low myopia (-5.00 D or less). A total of 52 patients who underwent bilateral, same day surgery with the EVO Visian ICL or the toric EVO Visian ICL were included. The target refraction in all cases was emmetropia, and all eyes (N = 104) had a preoperative DCVA of 20/20 or better. At least 1-year follow-up was available for all patients.
The mean age of patients was 27.36 ±3.5 years (range, 18–35 years*), and the mean refractive spherical equivalent (MRSE), the mean sphere, and the mean cylinder were -3.43 ±0.80 D (range, -4.88 to -1.75 D), -3.09 ±0.89 D (range, -4.75 to -1.00 D), and -0.69 ±0.64 D (range, -3.25 to 0.00 D), respectively. At 1-year postoperative, the average deviation from intended correction was -0.17 ±0.22 D (range, -0.50 to 0.75 D). Cumulative distance UCVA and change in CDVA are shown in Figures 2 and 3. It is worthwhile to note that no eyes lost any lines of distance BCVA, 42% gained 1 line, and 6% gained 2 lines. Only one eye experienced lens rotation, which was due to an undersized lens being implanted. This lens was exchanged for one of adequate size at 3 months postoperatively; ICL exchange, when needed, is simple and safe to perform.
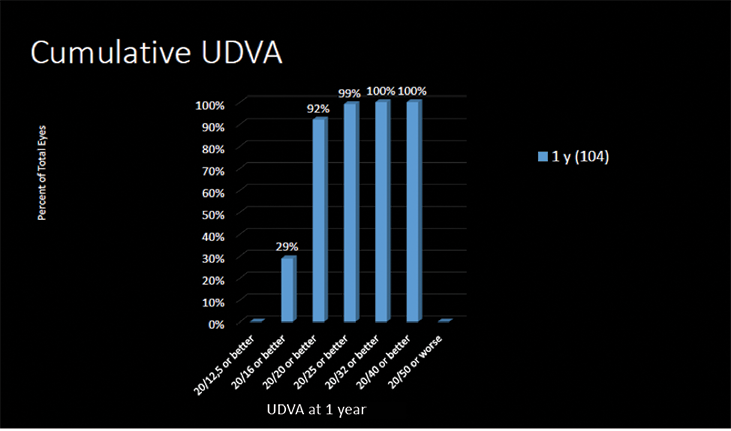
Figure 2. Cumulative distance UCVA from preoperative to 6 months postoperative.
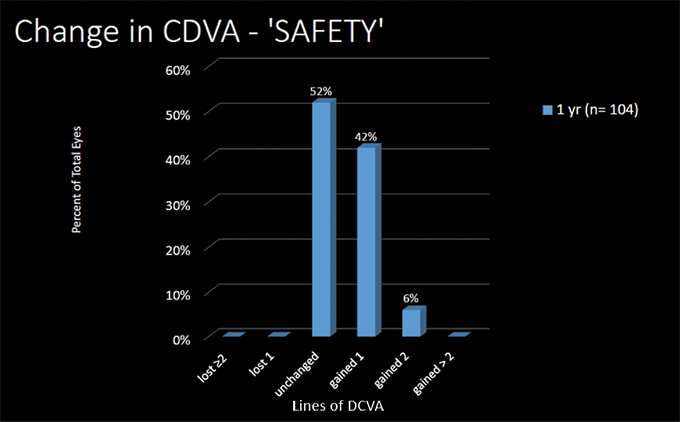
Figure 3. Change in distance BCVA at 1 year postoperative.
In the astigmatic eyes that received the toric EVO Visian ICL, the mean cylinder improved from -0.92 ±0.93 D preoperative to -0.33 ±0.46 D by 1 year postoperative. Further, the root-mean-square (RMS) higher-order aberrations and coma over time were relatively stable, and by 1-year postoperative, were back to preoperative levels (Figures 4 and 5).
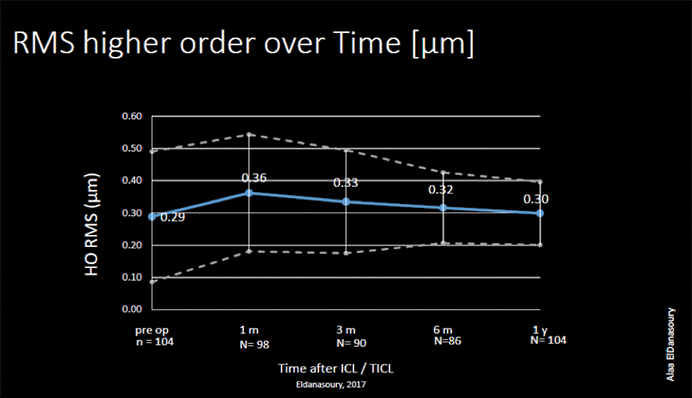
Figure 4. Root-mean-square of higher-order aberrations over time.
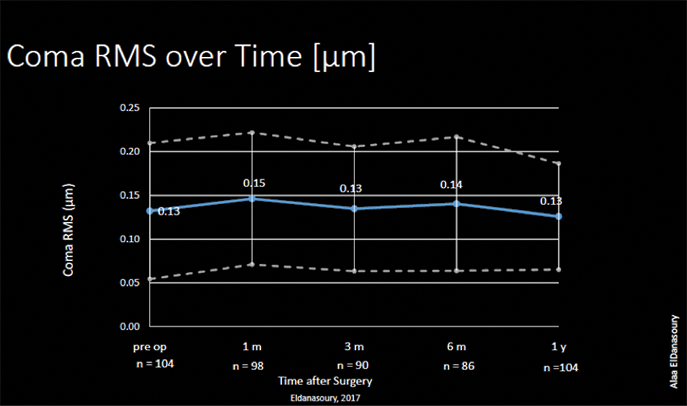
Figure 5. Root-mean-square of coma over time.
CONCLUSION
Our recent results help to prove that the EVO Visian ICL is a viable option for refractive correction in a wider range of patients, including a wider distribution of ages and a wider distribution of refractive correction. I am now able to treat low myopes (below -5.00 D) with the EVO Visian ICL, and this is a welcomed evolution in patient care. I have complete confidence in the surgical reproducibility of the EVO Visian ICL, I have complete confidence in selecting the proper sizing of the lens, and I have complete confidence in the toric lens’ design to ability to correct astigmatism.

* This is outside the approved age range for Saudi Arabia



