



The demand for intraocular procedures is on the rise. The two main contributors to the recent spike in cataract surgery volume are an aging population1 and a backlog of patients who deferred or delayed surgery owing to the COVID-19 pandemic.2 Additional factors include the growing potential for superb visual outcomes, spectacle independence, and a predictable and easy recovery after surgery. In Belgium, where I practice, an increasing number of patients are interested in elective intraocular procedures such as refractive lens exchange and phakic IOL implantation.
In my opinion, there is no reason why any of these surgeries cannot be performed as a same-day bilateral procedure as long as proper protocols are respected and patients are carefully selected. In fact, instituting sequential bilateral intraocular surgery could help to alleviate the backlog of patients and long waitlists for surgery, both of which are likely to be exacerbated by a growing disparity between the demand for surgery and the supply of cataract surgeons in the workforce.3
BILATERAL CATARACT SURGERY
Immediately sequential bilateral cataract surgery (ISBCS), although highly debated, is growing in popularity. The most obvious arguments for ISBCS and other bilateral intraocular surgery procedures are the following4:
• No disruption of stereopsis;
• A lower risk of complications associated with general anesthesia;
• Faster visual rehabilitation;
• Better patient compliance due to one versus two postoperative drop regimens;
• Cost and time savings;
• A quicker return to normal life for patients; and
• Fewer postoperative follow-up visits.
Proponents of ISBCS also argue that performing cataract surgery on both eyes of a patient on the same day has benefits for the clinic, including greater workflow efficiency, shorter OR turnover time, and fewer patients in the practice on a given day.5,6 Opponents of ISBCS point to the risk of bilateral endophthalmitis,4,5,7 an inability to adjust refractive outcomes for the second eye based on outcomes for the first eye, and unfavorable financial reimbursement.
Articles in the peer-reviewed literature have eased concerns over the risk of bilateral endophthalmitis.4,5,7 Two studies found that the rate of endophthalmitis was similar after ISBCS compared to delayed bilateral sequential cataract surgery (DBSCS) as long as strict safety protocols were observed.4,5 In other words, if surgery on each eye is treated as a separate surgical procedure and separate sterile setups are initiated such as rescrubbing in between eyes, then ISBCS can be as safe as DBSCS. Medications from different manufactured lots should be used for each eye during ISBCS to reduce the risk of bilateral infection.
Many physicians have also shown that, for routine patients, both ISBCS and DBSCS achieve good refractive outcomes.4,5 Further, ISBCS may be the better option for patients with significant refractive errors because it can prevent postoperative anisometropia and restore postoperative depth perception.
Patient selection is crucial to the success of ISBCS. Those at increased risk of unpredictable refractive outcomes (eg, patients with high myopia, hyperopia, or a history of refractive surgery) often do better with DSBCS. Likewise, DSBCS tends to be a better choice for patients at increased risk of postoperative complications such as those with dense cataracts or a history of diabetic retinopathy, uveitis, and corneal endothelial dystrophy.
BILATERAL PHAKIC IOL SURGERY
Immediately sequential bilateral implantation of phakic IOLs is performed less often than ISBCS, but an immediately sequential protocol for the former surgery can safely offer many of the same advantages and benefits to patients and clinicians as an immediately sequential protocol for the latter procedure.
The rate of endophthalmitis associated with the implantation of an Evo ICL (STAAR Surgical) is low.8 Prophylaxis is key. Similar to with ISBCS, povidone-iodine is applied to the eyelid (10%) and ocular surface (5%) at both 15 and 3 minutes before bilateral Evo surgery and reapplied immediately after surgery.9,10 To implant the Evo, one paracentesis incision and a 2.6-mm main incision are created, and intracameral cefuroxime 1 mg/0.1 mL is instilled.
As during ISBCS, I use medications from different manufactured lots, and I change my gown and gloves and rescrub in between surgery on the first and second eyes. The IOP is checked 1 hour after surgery, and patients receive 250 mg acetazolamide postoperatively.
Following this protocol helps me to perform bilateral Evo surgery safely and predictably and achieve proper vaulting without the need to adjust refractive outcomes for the second eye based on results with the first eye. I analyzed the results of 1,469 eyes in which I performed immediately sequential bilateral implantation of the Evo ICL. Of these, 306 were observed for 3 years or more. The attempted versus achieved refractive outcome in all eyes was excellent (Figure 1). Of the eyes that were monitored for at least 3 years, 97% achieved 20/20 UCVA and 57% achieved 20/16 UCVA (Figure 2).
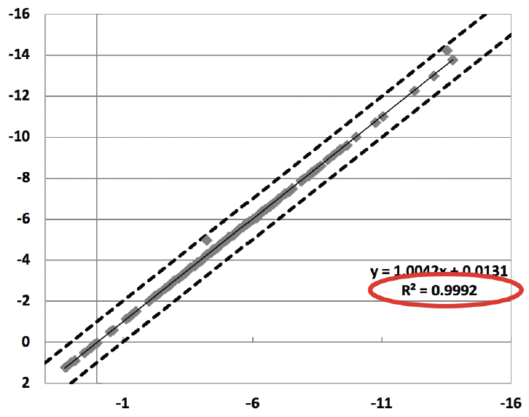
Figure 1. Attempted versus achieved refractive outcome in eyes that underwent immediately sequential bilateral implantation of the Evo ICL.
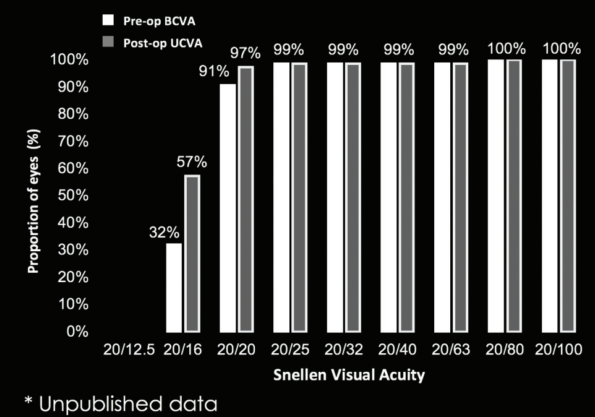
Figure 2. Cumulative UCVA of 306 eyes with more than 3 years of follow-up.
There is a growing body of evidence that immediately sequential bilateral intraocular surgery is safe and advantageous. When safety protocols are respected, the risks of bilateral endophthalmitis and other postoperative complications are low.4,5,11 Immediately sequential bilateral intraocular surgery can also enhance the patient experience by reducing the number of office visits and making the postoperative treatment course easier. Offering patient-centered care is more important than ever before. I believe that immediately sequential bilateral intraocular surgery is essential to the success of ophthalmologists in the current health care model.12,13 I hope that, in time, the remaining barrier to adoption—reimbursement—is resolved.
1. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye preferred practice pattern. Ophthalmology. 2022;129(1):P1-P126.
2. Aggarwal S, Jain P, Jain A. COVID-19 and cataract surgery backlog in Medicare beneficiaries. J Cataract Refract Surg. 2020;46(11):1530-1533.
3. Health Resources and Services Administration. National and regional projections of supply and demand for surgical specialty practitioners: 2013-2025. Published 2016. Accessed November 23, 2021. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/data-research/surgical-specialty-report.pdf
4. Singh R, Dohlman TH, Sun G. Immediately sequential bilateral cataract surgery: advantages and disadvantages. Curr Opin Ophthalmol. 2017;28(1):81-86.
5. Singh G, Grzybowski A. Evolution of and developments in simultaneous bilateral cataract surgery. Update 2020. Ann Transl Med. 2020;8(22):1554.
6. Masket S. Same day bilateral cataract surgery-who benefits?. Ophthalmology. 2021;128(1):11-12.
7. Arshinoff S, Bastianelli P. Incidence of postoperative endophthalmitis after immediate sequential bilateral cataract surgery. J Cataract Refract Surg. 2011;37:2105-2114.
8. Allan B, Argeles-Sabate I, Mamalis N. Endophthalmitis rates after implantation of the intraocular Collamer lens: survey of users between 1998 and 2006. J Cataract Refract Surg. 2009;35:766-769.
9. Levinson JD, Garfinkel RA, Berinstein DM, Flory M, Spellman F. Timing of povidone-iodine application to reduce the risk of endophthalmitis after intravitreal injections. Ophthalmol Retina. 2018;2(7):654-658.
10. Haripriva A, Baam ZR, Chang DF. Endophthalmitis prophylaxis for cataract surgery. Asia Pac J Ophthalmol. 2017;6(4):324-329.
11. Herrinton LJ, Liu L, Alexeeff S, Carolan J, Shorstein NH. Immediate sequential vs delayed sequential bilateral cataract surgery retrospective comparison of postoperative visual outcomes. Ophthalmology. 2017;124(8):1126-1135.
12. Wang H, Ramijiani V, Raynor M, Tan J. Practice of immediate sequential bilateral cataract surgery (ISBCS) since COVID-19: a patient and surgeon survey. Eye. 2022;36:888-890.
13. Bhalla JS, Zakai MU, Mehtani A. Immediate sequential bilateral cataract surgery and its relevance in COVID-19 era. Indian J Ophthalmol. 2021;69(6):1587-1591.