

Improved Astigmatism Management With Catalys’ Laser Marking and Registration
H. Burkhard Dick, MD, PhD, FEBOS-CR

Accurately correcting astigmatism at the time of cataract surgery is essential for good visual outcomes,1 but it has always posed challenges. For example, the efficacy of toric IOLs is dependent upon a precise preoperative measurement of the axis of astigmatism followed by correct placement of the IOL on that axis during surgery. Each degree of rotational misalignment of a toric IOL reduces its effect by 3.3%.2 This is of particular concern with high-powered toric IOLs. Limbal relaxing incisions, which in my practice have been replaced by femtosecond laser intrastromal arcuate incisions, provide an opportunity to address lower levels of astigmatism but also require exact placement.
The new cOS 6.0 software for the Catalys Precision Laser System (Johnson & Johnson Vision) facilitates both kinds of correction by enabling the direct importation of preoperative data from the Cassini (i-Optics), the biomorphometric intraoperative registration of iris features, and precise laser marking. I have been testing versions of this software for years and am now participating in a controlled clinical trial of the commercially available version.
MORE PRECISE MARKING
Historically, surgeons have marked the horizontal axis preoperatively and the target axis relative to the horizontal mark with an additional instrument intraoperatively. Some directly mark the target axis preoperatively, but any form of manual ink marking introduces the potential for error because of the thickness of the ink mark and rotation or tilt introduced by the marker. One study3 estimated that ink marking can contribute to a misalignment of nearly 5°. Additionally, surgical delays and epithelial erosion can cause the marks to fade or disappear, leaving the surgeon guessing in the OR. The latest Catalys software eliminates the need for manual marks. Instead, it compares the pre- and intraoperative iris anatomy data and compensates for tilt and rotation so that the laser marks are perfectly aligned to the steep meridian and the target axis.
Tim Schultz, MD, and I described this laser-assisted marking technique for toric IOL alignment several years ago.4 The alignment marks are easy to visualize under an operating microscope and can be seen for several months postoperatively, which is—in the rare case—helpful in troubleshooting the source of a residual error. Patients do not experience foreign body sensation, peripheral glare, or epithelial defects near the marks.4
MORE EFFICIENT WORKFLOW
Linking preoperative diagnostic information to the laser minimizes data entry and eliminates several steps in the planning process for toric IOLs and arcuate incisions (Figure 1). The examination, evaluation, and treatment planning are all done preoperatively with the Cassini, and these data are imported via a wireless connection or USB drive to the laser. Toric calculators and the Donnenfeld incisional nomogram (which we use at 90% for effective intrastromal incisions) are integrated into this system. There is no need to use a separate online calculator and manually enter that information into the laser system. Nor is one hampered by technological challenges such as a firewall or plug-in issue or spotty internet access in the clinic.
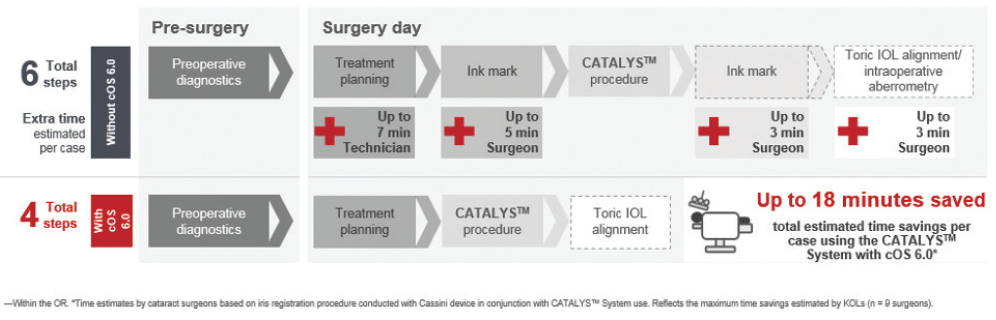
Figure 1. More efficient arcuate incision workflow.
ENHANCED SAFETY AND ACCURACY
Iris detection is a big step forward in the personalization and individualization of laser arcuate incisions. The intraoperative iris features are referenced and adjusted to those from preoperative Cassini tomography to identify the target location for the incisions (Figure 2). This avoids problems that can arise from cyclorotation as well as docking-related tilt, which is otherwise impossible for the surgeon to identify and compensate for.
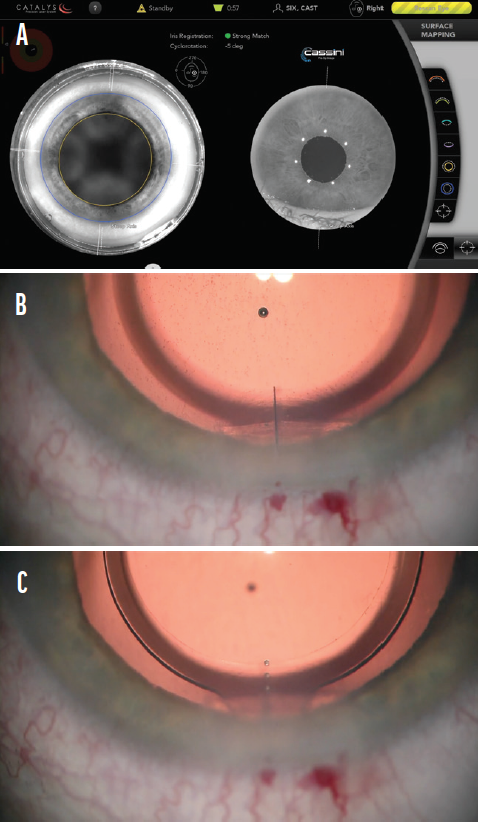
Figure 2. Intraoperative iris registration demonstrates a strong match between the preoperative examination and intraoperative situs. The incision mark is aligned accordingly (A). Intraoperative view of the corneal laser cataract surgery mark based on the individual iris registration (same eye, B). Intraoperative view of the IOL torus aligned to the corneal laser cataract surgery mark (same eye, C).
Figures 1 and 2 courtesy of H. Burkhard Dick, MD, PhD, FEBOS-CR
As a sophisticated biomorphometric tool that is used for a sensitive application such as passport control, iris detection largely eliminates the potential to accidentally operate on the wrong eye or wrong patient. These enhancements in precision and safety are steps in the right direction for surgeons who continually want to perfect their cataract surgery and astigmatism management outcomes.
1. Watanabe K, Negishi K, Kawai M, Torii H, Kaido M, Tsubota K. Effect of experimentally induced astigmatism on functional, conventional, and low-contrast visual acuity. J Refract Surg. 2013;29(1):19-24.
2. Ma JJ, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631-1636.
3. Visser N, Berendschot TTJM, Bauer NJC, Jurich J, Kersting O, Nuijts RMMA. Accuracy of toric intraocular lens implantation in cataract and refractive surgery. J Cataract Refract Surg. 2011;37(8):1394-1402.
4. Dick HB, Schultz T. Laser-assisted marking for toric intraocular lens alignment. J Cataract Refract Surg. 2016;42(1):7-10.
High Cutting Precision With the Femto LDV Z8
Bojan Pajic, MD, PhD, FEBO

Advances in femtosecond laser design include improvements in operation and performance. Recent innovations on the Femto LDV Z8 (Ziemer) are discussed herein.
The cutting effect of femtosecond laser pulses is achieved by placing individual spots next to or overlapping each other (Figure 3). The precision of the cut is achieved with minimal cavitation bubble volume, and it increases with the use of shorter pulses and by achieving a smaller focal volume (Figure 4). Conversely, if the focal volume is reduced, a higher number of pulses is required to achieve the same section size. This is achieved by increasing the repetition rate of the laser to keep the treatment time short.

Figure 3. Individual laser spots are applied side by side with possible tissue bridges (A). Overlapping laser spots promote continuous tissue cutting (B).
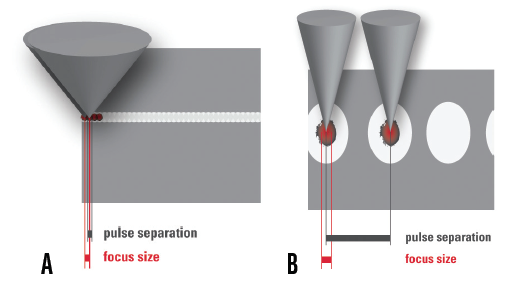
Figure 4. A shortened pulse duration causes a reduced energy transport in the tissue and thus a reduced probability of a side effect (A). The numerical aperture is decisively responsible for the size of the laser spot (B).
The quality of the cut also depends on the spatial distance between the laser pulses as a function of their energy. It has been shown that a pulse duration of 150 to 200 femtoseconds is best for microsurgical applications.1 The only high-frequency, low-energy femtosecond laser available today is the Femto LDV. It produces a pulse energy in the nanojoule range and has tissue-adapted power delivery. In other words, the more posterior the cut is placed, the more energy is used, and the more anterior the cut is placed, the less energy is used. In my experience, the power delivery system of the Femto LDV Z8 improves cut quality.
GREATER CUT QUALITY
The latest software upgrades to the Femto LDV Z8 have improved cut quality and precision and reduced procedural time. As a result, less time is required for the capsulotomy, and cutting quality, surgical efficiency, and the speed of lens fragmentation have improved, especially with thicker lenses. These factors contribute to an approximately 33% reduction in vacuum time. In my surgeries, it takes 2 minutes and 15 seconds on average for the total pretreatment or suction time, including capsulotomy, lens fragmentation, and creation of clear corneal incisions.
Another important improvement is the additional information now included in the platform’s OCT system. The meridians on intraoperative OCT are clearly outlined and color coded, which is helpful for orientation (Figure 5). Furthermore, the software now allows me to see on the monitor where the laser is currently cutting. This is particularly helpful for capsulotomy creation and lens fragmentation. The time it takes to generate the OCT images during creation of the arcuate incisions has also decreased, reducing procedural and vacuum times. As a safety feature during arcuate incision creation, the OCT system scans centrally and right to left to counteract a potential perforation.
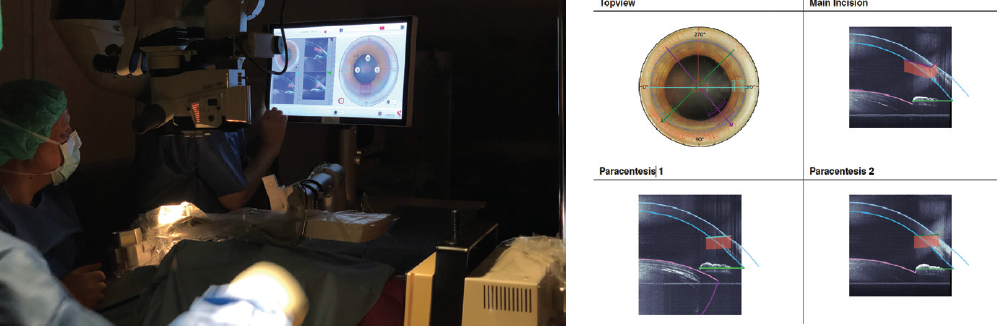
Figure 5. The meridians in the OCT scan are clearly outlined in color coding, which is helpful for orientation.
Figures 3–5 courtesy of Bojan Pajic, MD, PhD, FEBO
Additional innovations include a faster switching time between cataract and cornea applications, which reduces waiting time; a more precise and smooth flap creation; an optimized deep anterior lamellar keratoplasty module with color coding; and the ability to perform mushroom deep lamellar keratoplasty. Last but not least, the lenticule extraction module is now more user-friendly.
CONCLUSION
The latest updates to the Femto LDV Z8 increase cutting precision and decrease vacuum time. Additional features make the platform’s cataract surgery applications even safer than before.
1. Lubatschowski H. Update on fs laser technology in ophthalmology. Klin Monatsbl Augenheilkd. 2013;230:1207-1212.
Improvements to the Lensar Enhance Surgical Adaptability
Robert J. Weinstock, MD

One of the many lessons I learned this past year is that adaptability is important. I discovered that I could change the way I practice in order to remain successful but that changing my capital equipment was not so easy. I have therefore never felt more confident about my decision 7 years ago to acquire a Lensar Laser System (Lensar) because the company is committed to innovation. Lensar has continually improved its system to adapt to surgeons’ changing needs and to meet patients’ rising expectations, with six upgrades since the product’s initial launch.
CATARACT DENSITY IMAGING
Cataract density imaging (CDI) is a great example of Lensar’s innovations. This feature has taken laser cataract surgery to a whole new level. Thanks to augmented reality that uses Scheimpflug imaging, ray tracing, and 3D modeling software, CDI can grade the cataract 1 through 5 and identify the location and density of the nucleus to optimize fragmentation. After imaging and grading the cataract, the CDI software automatically adapts and recommends the most efficient fragmentation pattern based on my preferences.
This is important for two reasons. First, it expedites lens fragmentation by using appropriate laser energy targeted to the densest part of the lens, which varies depending on what grade of cataract is present. Second, it significantly limits or eliminates phaco energy, which improves visual outcomes on postoperative day 1 and speeds up recovery. Other femtosecond laser platforms that use OCT imaging do not have the resolution or imaging capable of grading cataract density and nucleus size.
INTELLIAXIS REFRACTIVE CAPSULORHEXIS
Preoperative information is imported wirelessly into the laser, which avoids the potential for transcription errors. The IntelliAxis Refractive Capsulorhexis marks the capsule and the cornea on the steep axis. I find this feature indispensable for cataract surgery on patients receiving a toric IOL and those receiving arcuate incisions to correct their astigmatism.
The system uses iris registration to eliminate cyclotorsion errors. Once docking of the laser is complete, iris registration is accomplished in less than 3 seconds. I no longer need to mark the cornea preoperatively or use other alignment tools during the cataract procedure. This is a huge time-saver.
FUTURE INNOVATION
Lensar plans to launch Ally, the market’s first cataract system that combines a femtosecond laser and phaco device, early next year. This will eliminate the need to roll patients between machines, and I am eager to evaluate the system’s impact on surgical efficiency and practice economics.
Digital Marking and Planning With the LenSx
O. Bennett Walton, MD, MBA

The use of a femtosecond laser for certain steps of the cataract procedure can enhance the surgical experience. When used in combination with other advanced technologies, femtosecond lasers can produce more predictable postoperative outcomes1 and offer additional value in the clinic for other ophthalmology procedures.
The increased predictability of spherical equivalent after laser cataract surgery is likely due to the standardized centration and sizing of the capsulotomy. Systems such as the LenSx (Alcon) deliver reproducible circumferential optic coverage, reduce lens tilt, and ensure a consistent effective lens position.1
In addition to cataract functionality, users who have upgraded to the latest LenSx software can use the laser to create flaps, sidecuts, tunnels, and pockets. The laser-assisted creation of tunnels and pockets is useful for the implantation of intrastromal corneal ring segments and presbyopia-correcting inlays.
Integration of the LenSx with the Verion Image Guided System (Alcon) increases accuracy and efficiency during surgical planning and execution. The company’s recent acquisition of the Argos biometer should facilitate digital marking and planning of astigmatic correction with toric IOLs and laser arcuate astigmatism correction.
1. Yeu E. Retrospective comparison of clinical outcomes associated with manual and femtosecond laser-assisted cataract surgery. Paper presented at the: 2018 ASCRS/AOA Annual Meeting; Washington, DC; April 13-17, 2018.
Centration, Comfort, and Versatility With the Victus
Mitchell Shultz, MD, and Abraham Chorbajian


It is hard to believe that nearly 10 years have passed since I (M.S.) first wrote about femtosecond lasers for cataract surgery. This technology had just debuted at the ASCRS Annual Meeting in San Diego and sparked my curiosity, and I was determined to learn everything I could about the various platforms. I spent the better part of the next 2 years doing research, watching other surgeons operate, meeting with industry executives, and visiting with the engineers who worked on all of the platforms available at the time. After completing my due diligence, I decided that the best platform for our center was the Victus femtosecond laser (Bausch + Lomb). It offered versatility for optimizing the accuracy and precision of corneal incisions and cataract surgery.
Nearly 8 years later, our practice has benefited greatly from this platform’s versatility for making consistent LASIK flaps, creating precise arcuate and corneal incisions, performing accurate capsulotomies, and presoftening cataracts with various fragmentation patterns (Figure 6).
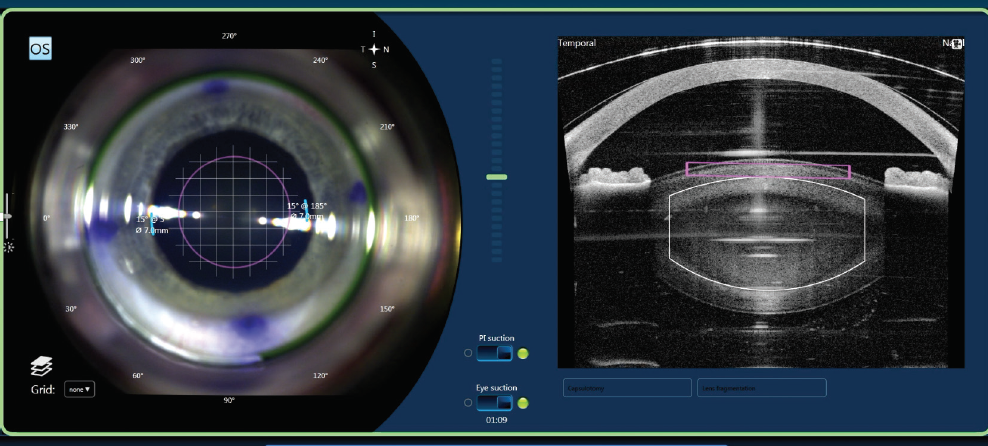
Figure 6. A treatment management screen of the Victus femtosecond laser.
Courtesy of Mitchell Shultz, MD
IMAGING AND GUIDANCE
The Victus is the only laser platform in its class to offer high-resolution, real-time OCT imaging and guidance. This makes it easier to plan and customize a grid fragmentation pattern. Coupling the Victus with the Stellaris Elite (Bausch + Lomb) for phacoemulsification has greatly reduced our total and effective phaco times by as much as 75% compared with traditional phacoemulsification without a femtosecond laser.
The live OCT imaging and state-of-the-art capsule scan allow us to optimize the position and effectiveness of capsulotomies and to customize the pattern of lens fragmentation to best suit each eye. A growing number of patients are choosing toric, accommodating, extended depth of focus, trifocal, and adjustable IOLs. Pairing these technologies with the Victus laser helps us to achieve the best possible refractive results for our patients.
CENTRATION AND COMFORT
The Victus can automatically center the procedure on the pupil, limbus, apex, or other positions, which facilitates the creation of well-centered corneal flaps and capsulotomies. With the soft silicone rim of the Victus Verafit patient interface, our patients do not complain about pain when their eyes are coupled to the laser. A recent redesign includes a curved liquid interface, which increases patient comfort and permits more flexible parameters for performing multiple procedures.
The combination of real-time live visualization, real-time OCT imaging, and the curved liquid interface help to minimize the risk of complications such as suction loss and conjunctival hemorrhage. The patient interface also provides optimal stability during creation of the LASIK flap, and it avoids posterior corneal folds, which can affect the anterior capsulotomy secondary to translation artifacts.
VERSATILITY
The integrated bed of the Victus allows cataract and corneal procedures to be executed under one workstation, and it can be used in conjunction with the Technolas Teneo excimer laser (Bausch + Lomb) to round out a complete refractive suite. This cost-effective versatility can enhance workflow and provide a high-quality surgical experience.
I (M.S.) typically spend less than 4 minutes total in the laser suite because most treatments take less than 2 minutes from start to finish. When I am operating, I generally perform a case with the Victus, go to the OR to perform phaco cataract surgery, and then return to perform another case with the Victus. This means I do not spend time waiting for the OR to be turned over.
