

OVDs for Surgery on Eyes With Dense Cataracts
Steve A. Arshinoff, MD, FRCSC

The first OVD to enter global markets was Healon (Johnson & Johnson Vision) in 1980. The introduction of OVDs enabled ophthalmic surgeons to reduce damage to the corneal endothelium during IOL implantation. The protection provided by Healon was thought to be a result primarily of its viscous-cohesive nature, which prevented IOL-corneal contact by permitting the AC to be deepened and stabilized in the presence of an open wound. Additional OVDs quickly appeared, including chondroitin sulfate 1 and 2, which were the precursors to Viscoat (Alcon), and hydroxypropyl methylcellulose.
Arguments about the relative benefits of different OVD properties began with their introduction and continue today because of the evolution of cataract surgical techniques—from intracapsular cataract extraction to extracapsular cataract extraction to phacoemulsification to laser cataract surgery—each of which changes the intraoperative environment in which OVDs are required. This article discusses phacoemulsification in 2021 and what I consider to be the optimal OVD strategy for removing a very dense cataract. I discussed the general proper use of OVDs in this space in 2019.1
Surgical requirements for a very dense cataract differ from the requirements for a moderate cataract chiefly because of the length of time that the protective OVD must remain present. The use of dispersive OVDs for surgery on eyes with dense cataracts has therefore been promoted, but this view is simplistic in my opinion.
Choose A Viscous-Cohesive OVD
The creation of the capsulorhexis requires maneuvering space and inducing pressure in front of the capsule (to prevent a tear-out). A viscous-cohesive OVD is best suited for this role, and for this reason, variants of the soft-shell technique remain preferable for dense (and other) cataracts.2 A dispersive OVD nestled against the endothelium provides prolonged retention and protection for the endothelium during long cases, and a viscous-cohesive OVD below the dispersive OVD allows pressure to be induced in front of the capsule. It is also helpful to leave a thin layer of balanced saline solution below the viscous-cohesive OVD, which may be used for a trypan blue solution in hypermature cataracts, or for a solution of xylocaine with phenylephrine or epinephrine (eg, Shugarcaine) to assist with maximal pupillary dilation.3
My preference is to use Viscoat as the dispersive OVD, Healon5 (Johnson & Johnson Vision) as the viscous-cohesive OVD, and my own xylocaine-phenylephrine formula below the OVDs as the third layer in what I term a trisoft shell technique (Figure 1).4
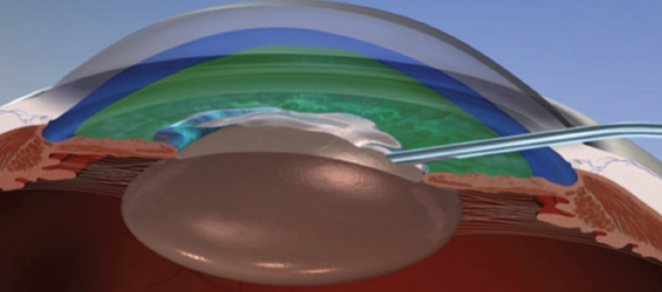
Figure 1. The layers of OVD in Dr. Arshinoff’s preferred trisoft shell technique.
Optimal Surgical Technique With OVDs
Cataract surgery is not just about OVDs, of course, so I will discuss them in the context of surgical technique. If the OVD shell comes apart and some amount of an OVD is lost, it is necessary to replace only the Healon5 because, in almost every instance, that is what has been unintentionally removed.
Capsulorhexis. After the AC has been stabilized with OVDs, the next step is to create an optimal capsulorhexis. When operating on an eye with a very dense cataract, the risk of rupturing the posterior capsule increases. Executing the first steps of surgery perfectly facilitates success with subsequent steps. The capsulorhexis should be well centered and no larger than 4.7 mm. This will allow the IOL to be easily captured in the capsulorhexis with excellent stability if the posterior capsule becomes torn. Capturing and stabilizing the IOL may be difficult or impossible with a larger capsulorhexis. The elasticity of the capsule must be taken into consideration during sizing (Figure 2).
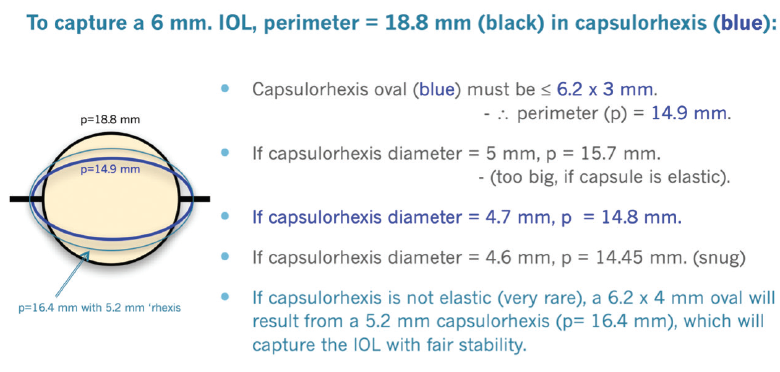
Figure 2. Dr. Arshinoff’s methodology for a proper capsulorhexis.
Hydrodissection. In dense cataracts, hydrodissection is best performed with a small-bore cannula. My preference is to use the Akahoshi II, 27-gauge beveld hydrodissection cannula (ASICO) to perform gentle subcapsular irrigation in a cortical-cleaving manner (with fluid directed upward and outward toward the anterior capsule) in all four quadrants. This approach takes a few seconds longer but leaves the OVDs undisturbed, and I find it results in a freely rotating nucleus within the capsular bag.
Phacoemulsification. When the cataract is dense, a high flow rate during phacoemulsification will wash out the OVDs. In contrast, a flow rate of 15 to 20 mL/min will disturb neither the Healon5 nor the Viscoat layer behind it, so phacoemulsification can be performed in the posterior quarter of the AC, behind the OVD layers. Resultant turbulence in the bag is equal to what would be achieved with a flow rate of 35 mL/min in the entire AC. Turbulence is the force that brings the nucleus to the phaco tip.
A phaco setting on continuously variable pulse minimizes chatter and maximizes the holding of the nucleus on the phaco tip. The nucleus is impaled just to the left of and beyond its center and held. The stabilized nucleus is chopped into six or eight segments (more pieces for dense lenses) using my favorite chopper, the Nichamin Quick Chopper (MicroSurgical Technology), and my phaco slice and separate technique.5 The bottle height is lowered to about 75 cm above the patient’s head or an IOP of 55 mm Hg on the Centurion Vision System (Alcon). (The IOP setting on the Centurion is approximately 75% of bottle height on other machines.) The purpose is to preserve the OVD structure, which protects the cornea.
With each slice of the nucleus, it becomes easier to make deeper and more complete slices into the dense nucleus. If left in situ, the retained segments help with nuclear rotation and preservation of a deep capsular bag as the entire nucleus is sliced.
IOL implantation. Once the nucleus is removed, irrigation and aspiration are easy to perform because the cortex is sparse and not sticky in dense cataracts. The second step of my ultimate soft-shell technique (IOL implantation) is to occlude the wound from the inside with a viscoadaptive OVD injected only in front of the capsular bag. The bag is then filled with balanced saline solution by injecting through the OVD. The IOL cartridge seals the wound and allows the IOL to be injected safely under the anterior capsule and into the bag while the OVD remains in front of the bag (Figure 3).
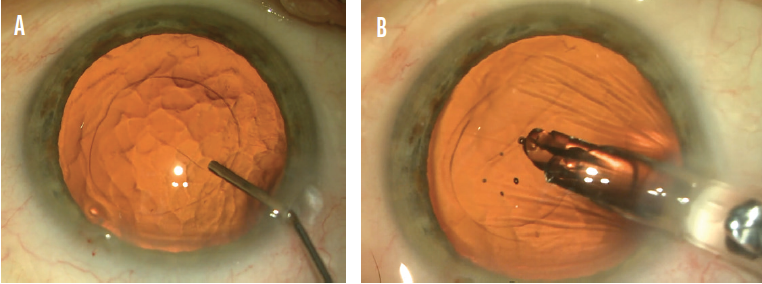
Figure 3. Dr. Arshinoff employs his ultimate soft-shell technique to implant an IOL. Surgery on an eye with a dense cataract entails injecting balanced saline solution through a viscoadaptive OVD, which has been placed only in front of the capsulorhexis, to fill the capsular bag (A). Then the IOL is injected through a cartridge, which blocks the incision, and into the capsular bag (B).
Figures 1–3 courtesy of Steve A. Arshinoff, MD, FRCSC
Conclusion
The goal with very dense nuclei is to keep the OVDs in place during phacoemulsification. The technique described herein achieves this goal and protects the cornea throughout the procedure. Nevertheless, my current favorite approach is to use a femtosecond laser to break up a very dense cataract, making phacoemulsification much easier and safer. Those cases require a different OVD strategy.6
1. Arshinoff SA. Tips for the proper use of OVDs. Cataract & Refractive Surgery Today. 2019;19(3). Accessed February 22, 2021. https://crstoday.com/articles/2019-mar/tips-for-the-proper-use-of-ovds/
2. Arshinoff SA, Norman R. Tri-soft shell technique. J Cataract Refract Surg. 2013;39:1196-1203.
3. Arshinoff SA. Ophthalmic viscosurgical devices for intumescent cataracts: pressure-equalized cataract surgery. J Cataract Refract Surg. 2015;41(7):1549-1550.
4. Arshinoff SA, Behndig A, Myers W. Intracameral medications for cataract surgery. Focal Points. American Academy of Ophthalmology. September 2018;Module 9.
5. Arshinoff SA. Phaco slice and separate. J Cataract Refract Surg. 1999;25(4):474-478.
6. Arshinoff SA. FLACS OVD press to prevent radial anterior capsular tears. Can J Ophthalmol. 2020;55:461-463.
My Preferred Chop Technique for Rock-Hard Cataracts
Maneesh Bapaye, MBBS, DNB(Ophth), FRCS(Ophth)*

Rock-hard cataracts are typically yellowish or brown in color, primarily due to the accumulation of the photo-oxidation pigment, urochrome. This type of cataract, sometimes called a catarock, is extremely dense and has a hard, brunescent nucleus. A rock-hard cataract presents a major challenge to surgeons that is often amplified by the presence of weak zonules and a thin posterior capsule. Additionally, the pupil may be small and rigid, and the endothelial cell count may be low. Careful management of each of these factors is necessary to minimize the risk of intra- and postoperative complications such as zonular dialysis, posterior capsular dehiscence, iris touch, wound burn, and delayed corneal decompensation.
Although I prefer the use of topical anesthesia in most cases, local anesthesia is indicated in certain situations such as the presence of a very small pupil, weak zonules, pseudoexfoliation, and lens subluxation and poor visibility due to a very dense arcus. If an extended surgical duration or problems with patient compliance are anticipated, I instead use peribulbar anesthesia.
Important Surgical Factors
Common techniques for surgery on eyes with a rock-hard cataract include creating a large capsulorhexis, employing a soft-shell technique to protect the endothelium, and placing pupillary expansion devices. In the absence of a good red reflex, I find it useful to stain the capsule with trypan blue dye before performing the capsulorhexis. Staining not only helps me to create the capsulorhexis, but it also improves visualization of the capsular margin, which helps to prevent inadvertent damage during phacoemulsification of the nucleus. Proper wound construction is extremely important to prevent iris prolapse, particularly if the tissue is floppy.
However, the crux of successful cataract surgery is effective management of the nucleus. It is important to minimize strain on the zonules and avoid trauma to the posterior capsule from a chopper or sharp-edged nuclear fragment. A direct chopping technique for hard cataracts is therefore preferred by most surgeons.
My Preferences
Instrumentation. I favor a long chopper, which can penetrate deep into lens matter and split the nucleus of a rock-hard cataract (Figure 4). I prefer to use a chopper with a sharp tip and inner edge, which facilitates penetration into lens material and splitting of the lens fibers. I use the Centurion phaco system, which sets the parameters for chopping hard cataracts at 50% power, a vacuum level of 450 mm Hg, and a flow rate of 28 mL/min. For the emulsification of nuclear fragments, power is usually between 65% to 90%, vacuum at 500 mm Hg, and a flow rate of 32 mL/min.
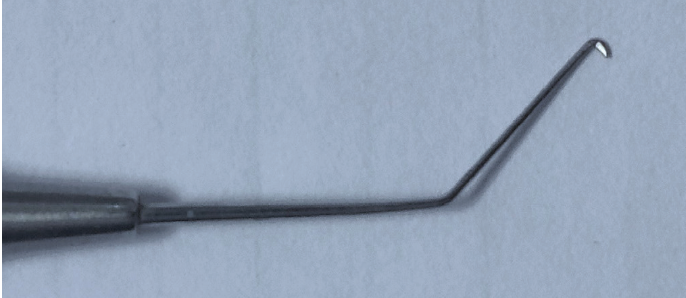
Figure 4. Dr. Bapaye uses a long chopper to penetrate deep into the lens and split the nucleus of a hard cataract.
Courtesy of Maneesh Bapaye, MBBS, DNB(Ophth), FRCS(Ophth)
Horizontal chop technique. For an eye with a hard cataract, I typically create a capsulorhexis ranging in diameter from 5.5 to 6.0 mm. This makes approaching the lens equator easier when using a horizontal chop technique—my preference. With this technique, lens material is held by the phaco probe, and the chopper is engaged as close to the lens equator as possible. After chopping in one axis, I rotate the nucleus by 180º and perform horizontal chop again before attempting a lateral split. This chop-rotate-chop maneuver dissects most of the lens fibers, and lateral separation places minimal stress on the zonules. I find this technique particularly useful in eyes with very weak zonules, as exemplified by the second case in the accompanying video.
Multilevel chop technique. I perform multilevel chop in select cases. This technique is useful for leathery, hard cataracts with a thick posterior plate. With multilevel chop, the phaco probe is engaged in progressively deeper levels of nuclear material as superficial fibers split while deeper fibers remain intact. Care must be taken not to cause posterior capsular dehiscence as the probe penetrates the nucleus. If the posterior plate is thick and difficult to crack, two instruments may be used.
After the nucleus has been divided into two hemi-nuclei, the horizontal chop technique is used to divide each hemi-nucleus into three or four pieces. A small piece of nucleus is emulsified soon after the initial chop, creating space in which to rotate other pieces and chop them. I usually lower the parameters to 50% to 60% torsional power and a vacuum level of 250 to 300 mm Hg when removing the last piece in order to avoid a sudden surge, potentially causing posterior capsular dehiscence.
Soft-shell technique. The endothelium is coated with a dispersive OVD, and a cohesive OVD is placed to flatten the anterior capsule or form the AC. Care must be taken to locate and remove every nuclear fragment, or corneal edema and inflammation may result.
Conclusion
Improvements in phaco technology have made surgery on an eye with a rock-hard cataract more routine. Nevertheless, it is prudent to have pupillary expansion devices, capsular hooks, endocapsular rings, and vitrectomy cutters accessible during these cases.
*Dr. Bapaye would like to thank Akshay G. Nair, MD, from Mumbai, India, for reviewing this article and for providing important feedback.
A Sharp Chopper in a Rock-Hard Nucleus Provides Many Advantages
Björn Johansson, MD, PhD, FEBO

A chopping approach offers many advantages over other methods of nuclear disassembly. Compared with sculpting techniques such as divide-and-conquer, chopping techniques put less stress on the zonules and capsule because the phaco tip holds the nucleus while the chopper is moved against it. Less ultrasound energy—and less surgical time—are required to emulsify and evacuate the lens material when it is chopped into smaller fragments.
For several years, I performed horizontal chopping using only a blunt chopper of the Nagahara type, regardless of cataract density. It wasn’t until after giving a presentation at a neighboring clinic’s video symposium that I learned the benefits of using a sharp chopper instead for these cases. After describing my technique for hard cataracts, several colleagues approached me to say something along these lines: “That was nicely handled, but why don’t you use a chopper with a sharp point instead? That will make it easier!”
Heeding their advice, I used a sharply pointed chopper and quickly discovered that it was much easier to get deeper into a hard nucleus using it. It was also at this time that I learned the vertical phaco chop technique, which I found allowed me to chop the nucleus without needing to move the chopper around the lens equator.
Phaco Chop Technique
I use a system with an internal vacuum pump and a dual linear footpedal to control ultrasound and vacuum independently. The main incision size is 1.8 mm. I find that a smaller incision limits fluid leakage, thereby stabilizing the AC. High levels of vacuum (maximum, 600 mm Hg) and ultrasound energy (usually 50%–60% maximum ultrasound compared to 20% for regular cataracts) are required in these cases, and stabilizing the chamber reduces the risk of significant postocclusion surge as the fragments pass through the phaco tip. In my experience, a bent Kelman tip is easier than other designs to bury at a steep angle toward the center of the nucleus before making the initial chop.
Many rock-hard cataracts are loosely attached—if at all—to the inside of the lens capsule and have only a thin layer of cortex. Before chopping starts, I remove the cortex as thoroughly as possible within the opening of the capsulorhexis, and I ensure that the nucleus rotates freely inside the capsule. With the phaco tip positioned just inside the capsulorhexis margin, I then activate ultrasound (in burst mode) and maintain a high level of vacuum to firmly fix the nucleus (Figure 5). In my experience, it is safe to let the tip sink into the nucleus until the irrigation holes on the sleeve are at least half buried. A large, hard cataract usually measures 5 to 6 mm from the anterior to the posterior pole. After the phaco tip is buried, ultrasound is halted while the vacuum level remains high.
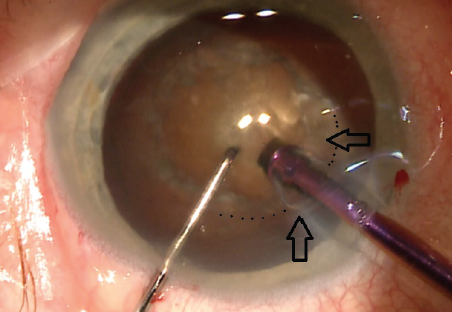
Figure 5. The beginning of Dr. Johansson’s chopping technique.
Courtesy of Björn Johansson, MD, PhD, FEBO
The sharp chopper is sunk into the nucleus at a point right inside the capsulorhexis margin and opposite the phaco tunnel while the vacuum level remains high and the phaco tip is occluded and fixing the nucleus. Next, the chopper is moved straight toward the phaco tip. Just before the instruments meet, the chopper is moved sideways to create a crack, although the nucleus typically does not split completely in half. By rotating the nucleus 180º and repeating the chop, however, it is possible to achieve complete separation of the two halves in most cases. It is often easier to create a complete crack that extends all the way to the posterior surface of the nucleus if lens chopping continues.
Depending on the sizes of the pupil and nucleus and the stability of the zonules and capsular bag, I create four quadrants or six or eight sectors. Smaller segments are more easily mobilized and brought to the tip of the phaco handpiece, with the tip placed in a safe central zone at the plane of the pupil. After the first pieces have been emulsified, it is often easier to emulsify the remaining parts a bit deeper in the capsule. Because hard cataracts require higher amounts of ultrasound energy, I increase the distance between the corneal endothelium and the phaco tip as needed.
Conclusion
For any surgeon who wants to transition from divide-and-conquer to a chopping technique, my advice is to become acquainted with both blunt and sharp choppers by using them regularly on every case. It may take a few tries to achieve a perfect chop. It took me four attempts. Only after some stop-and-chop surgeries where I divided the lens into two heminuclei after sculpting one initial trough did I start to become comfortable using a chopper and see success. Since then, I have never looked back.
How to Avoid Capsular Block Syndrome
Ozana Moraru, MD

Hydrodissection is required during most cataract procedures. This step assists with the separation of the nucleus and epinucleus from the peripheral capsular bag, and it facilitates the safe rotation of the IOL and the efficient completion of lens fragmentation and removal.
Capsular block syndrome (CBS) can occur if hydrodissection is performed aggressively and causes a sudden accumulation of fluid in the capsular bag. The fluid buildup pushes the lens anteriorly onto the anterior capsule, closing the capsulotomy, causing a rapid increase in pressure in the bag, and distending the posterior capsule. In some cases, the posterior capsule will rupture because of the pressure.
This article shares my preferred techniques for preventing CBS during hydrodissection in an eye with a mature cataract. Some are also summarized in the accompanying sidebar at the bottom of this page.
STANDARD TECHNIQUE
I favor an Akahoshi hydrodissection cannula (ASICO) because of its bent tip, which facilitates its insertion around the lens equator. The instrument can also be used to rotate the nucleus efficiently. When introducing the cannula, the wall of the incision is indented to release a small amount of OVD in order to avoid hyperpressure in the AC and capsular bag. The cannula enters the eye with its tip positioned horizontally under the continuous curvilinear capsulorhexis (CCC) at the 6 clock position, opposite the main incision, The anterior capsule is lifted slightly, and then the tip is rotated until it is positioned vertically around the lens equator (Figure 6).
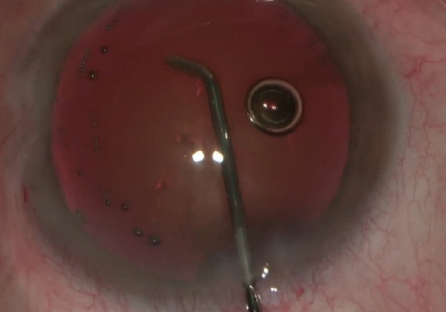
Figure 6. An Akahoshi cannula is introduced with the bent tip positioned horizontally.
Next, the least amount of balanced saline solution possible is slowly but firmly injected to produce a fluid wave between the nucleus and the posterior capsule. If the wave is not visible because of an absent red reflex or a small pupil, I watch for minimal elevation of the nuclear pole in the sector where fluid is injected while keeping the CCC margin slightly elevated. The fluid will therefore accumulate primarily behind the lens, and excessive fluid will flow forward into the AC.
The use of a 1-mL glass syringe can be helpful to control the gentle, continuous pushing of the plunger and avoid unwanted, irregular flushing. It may also be easier for a surgeon to sense the flow of balanced saline solution from a small syringe. A single-point injection is typically enough to produce complete hydrodissection of a soft cataract and often of a hard cataract. If a single-point injection does not induce complete hydrodissection, I perform single-point injections in several quadrants until I see a wave of balanced saline solution or the nucleus is slightly dislodged in the capsular bag. The same cannula is used to rotate the nucleus by vertically repositioning the bent tip. If the nucleus is not loose when rotated, balanced saline solution is delivered to one of the other injection points, and rotation is attempted again.
Techniques for Avoiding Capsular Block Syndrome with a Rock-Hard Cataract
- Swiping technique for hydrodissection. A minimal volume of balanced saline solution is injected before the tip of the cannula reaches the equator while the cannula swipes under the two halves of the continuous curvilinear capsulorhexis and gently pushes downward on the lens to allow the balanced saline solution to flow toward and beneath the equator.
- Capsular hooks on the anterior continuous curvilinear capsulorhexis. By lifting the anterior capsule, hooks create space that allows the egress of balanced saline solution. Thus, capsular block syndrome can be avoided even when aggressive hydrodissection is required.
- Phacoemulsification without nuclear rotation. If the placement of hooks does not allow safe and complete hydrodissection, phacoemulsification may be started without nuclear rotation. Splitting the nucleus and removing a small fragment creates space for the injection of balanced saline solution, which will complete the hydrodissection without the risk of trapping the fluid behind the lens with capsular block.
TECHNIQUES FOR MATURE CATARACTS
Slight modifications are required to prevent CBS during hydrodissection when the cataract is mature.
Rock-hard nucleus and white cortex. Hydrodissection is quite simple because the soft cortex occupies less volume in the bag than would solid cortex. Moreover, soft cortex tends to egress from the bag during creation of the CCC, which relieves pressure in the bag. Therefore, in these cases, a single-point injection of a minimal amount of balanced saline solution is typically sufficient for hydrodissection to be completed and the nucleus to be rotated easily.
If the pupil is small, insertion of the cannula tip can stop immediately after it passes the CCC (under the anterior capsule), and fluid is injected from there. The bent tip is kept horizontal so that fluid is directed toward the equator (Figure 7). Alternatively, a pupillary expansion device may be employed.
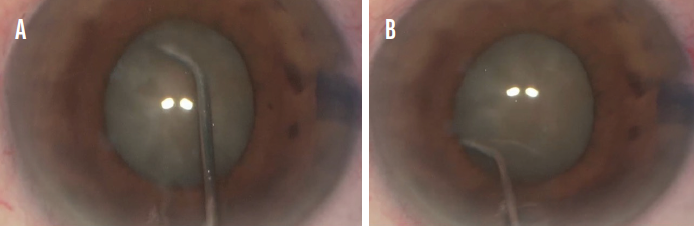
Figure 7. Dr. Moraru keeps the cannula tip horizontal and distanced from the equator (A) but under the anterior capsulorhexis (B) while balanced saline solution is injected.
White intumescent cataract. This requires special consideration because of its association with high IOP, a condition called secondary phacolytic glaucoma (Figure 8). Reduced space in the AC increases surgical complexity. The use of copious amounts of an OVD is required to protect the endothelium, deepen the AC, and control the CCC. Even the injection of a minimal amount of balanced saline solution can be dangerous because of the resultant increase in IOP in both the AC and the bag. If the entire lens and the CCC move forward, the AC flattens, and egression of the OVD is observed after the single-point injection of a minimal amount of balanced saline solution, I stop the hydrodissection and begin phacoemulsification. At this point, the goal is to create space by aspirating the cortex and creating the first split in the nucleus before hydrodissection continues.
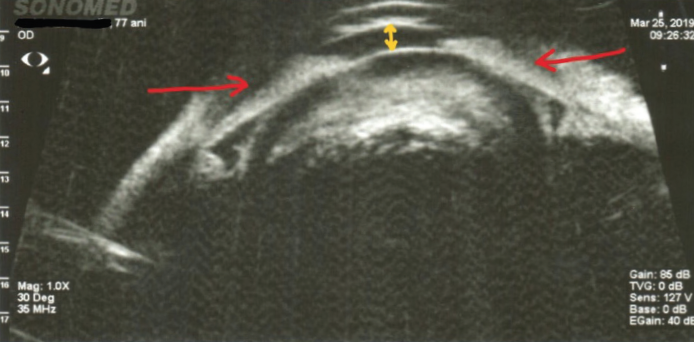
Figure 8. A hypermature intumescent cataract with phacomorphic glaucoma.
Morgagnian cataract. Although this type of cataract has a rock-hard nucleus, hydrodissection is generally easy, and there is no risk of CBS because of the completely liquefied cortex.
Rock-hard nucleus with epinucleus and cortex in a single block. Hydrodissection is challenging in these eyes because there is no space between the lens block and the capsular bag. If too little balanced saline solution is used, complete hydrodissection is impossible; if too much is used, pressure in the bag increases along with the risk of CBS. These eyes also often have pseudoexfoliation syndrome, weak zonules, a small pupil, and intraoperative floppy iris syndrome. Complete hydrodissection and rotation of the nucleus are required to increase the safety of the remaining steps of the procedure.
In these cases, a single-point fluid injection is never enough. At minimum, I administer an injection in each quadrant, including the subincisional area (Figure 9). In eyes with less space, such as those with a flat AC or a massive or adherent hard lens, I do not perform an injection directly in the equator. Instead, I use what I call a swiping technique. It entails advancing the cannula under the AC, continuously injecting a minimal amount of balanced saline solution, keeping the bent cannula tip horizontal under the left half of the CCC, and swiping the tip under the anterior capsule. The process is repeated for the right half of the CCC. While swiping the cannula, I also push it against the lens to create a small space, which facilitates fluid migration to the equator and beyond. The lens is also rotated at least few degrees. I repeat these maneuvers two or three times on both sides until the nucleus has been released.
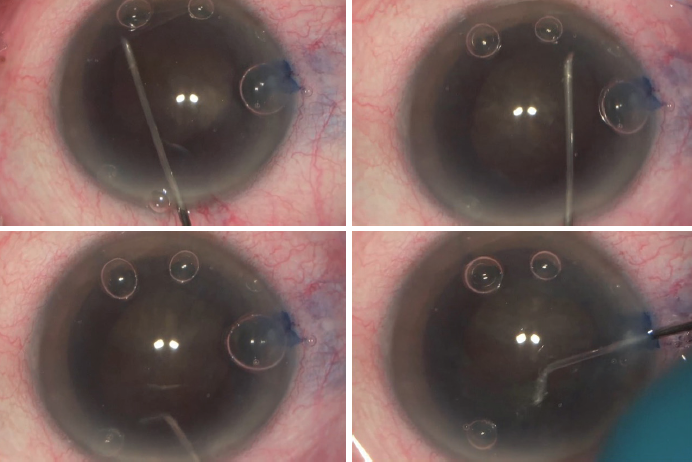
Figure 9. Several single-point injections of balanced saline solution directed to the equator in each quadrant.
If rotating the nucleus is difficult, hydrodissection is halted, and hooks are placed on the CCC to lift the anterior capsule and create more space between the lens and the bag (Figure 10). This allows more aggressive hyrodissection and, potentially, fluid reflux. In this way, CBS is avoided even when a higher volume of balanced saline solution is required. Moreover, nuclear rotation is much easier under hooks because they stabilize the bag as well.
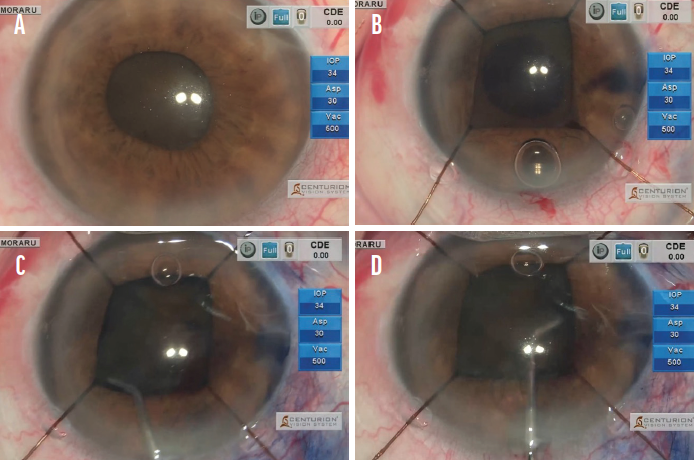
Figure 10. An eye with a rock-hard cataract, small pupil, and pseudoexfoliation syndrome (A). Iris hooks are used from the outset of the case, and they are later moved to the CCC (B) to facilitate safe hydrodissection (C and D).
Figures 6-10 courtesy of Ozana Moraru, MD
If the nucleus still seems to be attached to the bag after the placement of hooks, I start phacoemulsification and split the nucleus without rotating it. As soon as the first free fragment is created, it is removed to create space for the completion of hydrodissection without the risk of CBS.
Laser cataract surgery in a rock-hard nucleus. During laser cataract surgery on an eye with a rock-hard nucleus, the bag has excess pressure before hydrodissection begins because air bubbles form after laser energy is released in the anterior chamber and capsular bag. In addition to minimizing the volume of balanced saline solution injected, I use the same technique to prevent capsular block syndrome as I would for the standard extraction of a mature cataract. I don’t try to extract the air bubbles from behind the lens because they can help with nuclear rotation.
Space Matters
Preventing and recognizing CBS is more challenging in eyes with mature cataract. The amount of space between the lens and the posterior capsule determines the risk of CBS during cataract surgery. Therefore, the optimal approach depends on the type of cataract and the amount of space between the lens and the posterior capsule.
A peripheral red reflex may be present in some eyes with a mature cataract, bu usually the red reflex is absent, and visualization of the fluid wave during hydrodissection is impossible. In this situation, employing the swiping technique for hydrodissection, placing hooks on the anterior CCC, and starting phacoemulsification without nuclear rotation are options that can help avoid CBS.
