


CASE PRESENTATION
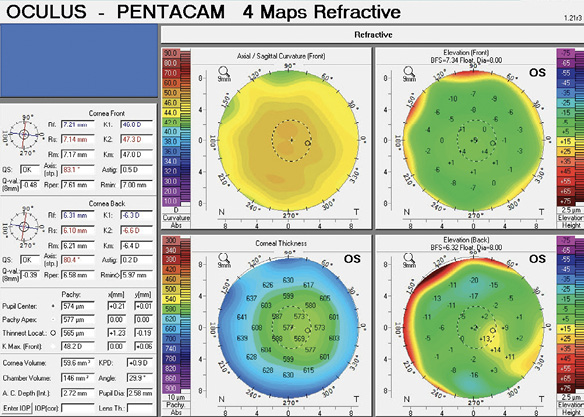
Figure 1. Preoperative measurements for the patient’s left eye with the Pentacam (Oculus Optikgeräte).
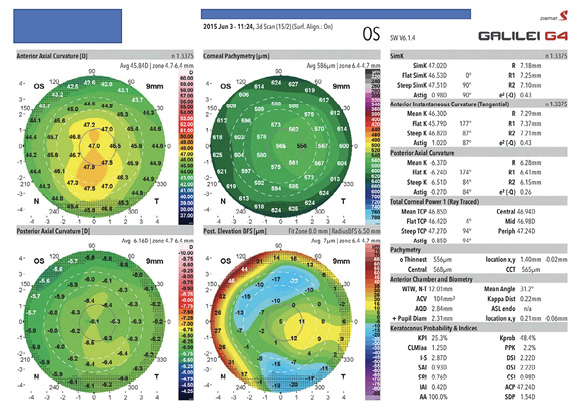
Figure 2. Preoperative tomography of the patient’s left eye with the Galilei G4.
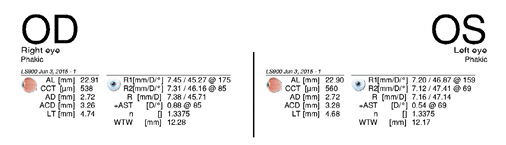
Figure 3. Preoperative biometry measurements obtained with the Lenstar.
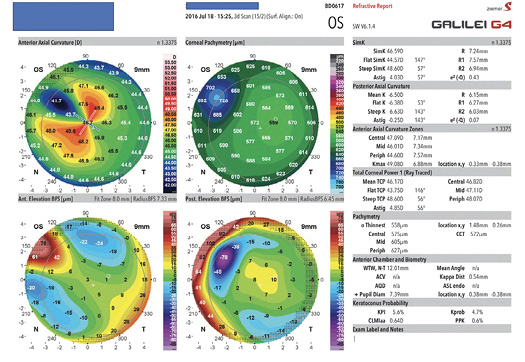
Figure 4. Biometry measurements obtained with the Lenstar 5 weeks after cataract surgery.
Figure 5. Tomography performed 5 weeks after cataract surgery. The primary incision is on the 145º to 150º axes.
—Case prepared by Alan N. Carlson, MD

JOHN A. HOVANESIAN, MD
The amount of astigmatic flattening caused by a corneal incision is related to three incisional factors: depth, length, and location. Incisions that are deeper, longer, and closer to the corneal apex cause greater flattening. Maximal topographic flattening appears over the incision itself, and curvature powers in the same meridian become greater at points closer to the central cornea. Based on Figure 5, which shows the area of maximal flattening 2 to 3 mm from the corneal apex, this patient’s laser cataract incision at the 145º meridian appears to have been quite central. This location is also where the previous hyperopic ablation would have caused the greatest corneal thinning. The combination of these two effects—a too central incision and a locally thin cornea—could easily account for the unexpectedly high degree of flattening induced by the cataract incision.
To manage this case, it would be reasonable to place a compression suture in the area of the corneal incision to reduce the local flattening. Although compression sutures are difficult to titrate, they can be reasonably precise when guided by intraoperative aberrometry—a technology that was available to the second surgeon. Also, although a compression suture might lose effect as it degrades over time, the suture would provide immediate relief and would alleviate the problem of irregular astigmatism at its source, instead of by flattening the cornea 90º away with further unpredictable incisions.
Another reasonable approach would be to exchange the existing IOL for a toric. This would be best executed after the refraction stabilized and would be a second-best approach because, unlike a compression suture, a toric IOL would not address the asymmetry of the incision-induced astigmatism.

A. JOHN KANELLOPOULOS, MD
The meticulous data presented indicate that the direction of the primary laser cataract incision is the main problem with the original cataract procedure on this patient’s left eye. This case highlights the importance of preoperative evaluations with multiple anterior segment diagnostic tests. For instance, corneal topography and/or tomography would have helped to pinpoint the problem here earlier. Aberrometry, moreover, would have helped if the large amount of cylinder in the eye was present intraoperatively.
For any pseudophakic patient with a nontoric IOL who has difficulty achieving good corrected distance visual acuity, I generally find that a trial with rigid gas permeable lenses can differentiate a corneal problem from other issues such as posterior capsular opacification, an epiretinal membrane, or cystoid macular edema. Several patients have presented to me as so-called cataract surgery failures who had mild undiagnosed keratoconus.
The sequence of events in this case suggests that the elevated IOP in the operated eye might have stretched the laser cataract incision, which was located in a region of the cornea that was potentially already biomechanically weak from the hyperopic LASIK procedure.
An IOL exchange would not have been my first choice if topography, tomography, and/or a contact lens trial revealed very high regular postoperative astigmatism. Suturing the cataract incision with several interrupted compression sutures might have been a simpler, less invasive, and more effective means by which to reduce the cylinder, improve visual function, and possibly allow adjustment of the final cylinder through titrated removal.
I am not an advocate of large AKs as a tool to correct 4.00 D of incision-induced cylinder (Figure 5) because their efficacy, even when performed with an accurate femtosecond laser, has been variable in my hands. The incisions may worsen dry eye symptoms, especially in female patients, and further weaken already disturbed corneal biomechanics.
If I did not choose to suture the stretched primary cataract incision, I would perform a LASIK enhancement (an old flap already exists in that eye, allowing ablation under the flap) or even surface ablation.

ALAN N. CARLSON, MD
The factors leading to a recommendation for IOL removal were murky and inconsistent. The spherical equivalent supports that the original IOL was the proper power for targeting intermediate and near vision. The power of the IOL also confirms this idea.
Correcting astigmatism requires identifying the cause or source, the magnitude, and the axis and assessing its stability. Whenever possible, it is best to correct a progressing problem at its location. Treating wound dehiscence with AK incisions made 90º away adds structural weakness to a problem that was caused by structural weakness. If a tire on my car were leaking air, my solution would not be to let air out of the other three tires. Suturing the wound would have been a better option in this case. A tight, deep suture that temporarily overcorrected the problem could be safely removed after 6 to 8 weeks, likely correcting the problem or at least vastly improving the situation.
A toric IOL would also be a reasonable option, but only if the astigmatism were regular and stable, which was not the case for this patient.
