
I am an anterior segment surgeon with a special interest in glaucoma surgery. My favorite surgical management techniques are deep sclerectomy and canaloplasty. The latter procedure is particularly fascinating to me; it offers equivalent IOP-lowering efficacy to traditional filtering surgery without the bleb-related complications. Ab externo canaloplasty is, however, technically challenging to perform. Several innovations over the years have helped to simplify the procedure, including the OMNI Surgical System (Sight Sciences). This technology has once again changed the way we can help our patients to decrease their dependence on medication with a much better safety profile.
BACKGROUND
Some years ago, it was proposed to use an ab interno approach to cannulate and viscodilate the Schlemm canal by using the same type of microcatheter from a standard canaloplasty procedure but without leaving the prolene suture inside the canal. In addition to lowering IOP, another advantage of ab interno canaloplasty is that it leaves the conjunctiva untouched and ready for other surgical interventions, including MIGS procedures.1,2 The main drawback of this approach, however, is that it was not easy to perform and required the surgeon to use both hands to manage the microcatheter in the anterior chamber.
The introduction of the VISCO 360 Viscosurgical System (Sight Sciences) and more recently the OMNI Surgical System has dramatically improved the ab interno canaloplasty technique. These devices are specifically designed for ab interno viscodilation of the Schlemm canal, enabling surgeons with experience in angle-based procedures to perform these techniques more efficiently than ever before.3
MY EXPERIENCE
I have been using an ab interno canaloplasty approach for almost 4 years, first with the VISCO 360 and now with OMNI. The technique is extremely efficient and intuitive. The OMNI device is easily inserted into the anterior chamber, through a 1-mm clear corneal incision (Figure 1), with a curved cannula tip filled with a high molecular weight OVD such as Healon GV (Johnson & Johnson Vision) or similar. A gonio lens with or without a handle is placed on the cornea to enable proper visualization of the angle. The tip of the cannula is then moved across the pupil, toward the iridocorneal angle, and the cannula tip is pressed against the trabecular meshwork (TM) to create a small opening in the Schlemm canal. The microcatheter is then inserted by turning the small wheel located on the handle of the device (Figure 2). Upon retraction of the microcatheter, the OVD is injected in a consistent and measured amount to dilate the Schlemm canal and address any possible herniations or blockages of the distal collector channels.
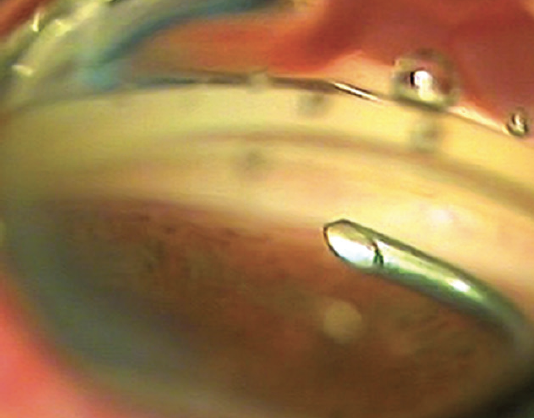
Figure 1. The curved cannula tip in the anterior chamber.
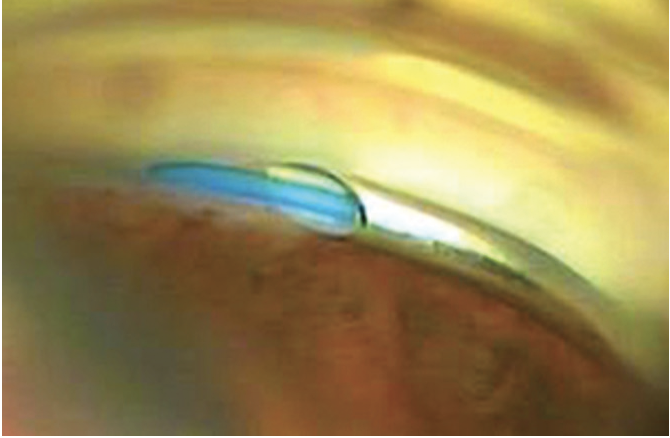
Figure 2. The microcatheter enters into the Schlemm canal, which was previously opened with the tip of the cannula.
The catheter is deployed within the Schlemm canal for 180° or one hemisphere at a time (Figure 3). The same maneuver can be repeated in the opposite hemisphere by removing the cannula from the anterior chamber (AC), rotating the cannula 180º, and reentering the AC to treat the remaining hemisphere. Once complete, the surgeon has circumferentially dilated the entirety of the canal. After completing the viscodilation, the cannula is then removed from the anterior chamber and the OVD is forced out by injecting balanced saline solution until it has been completely removed.
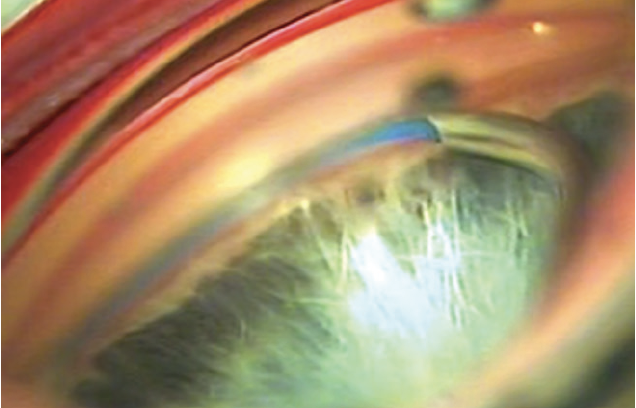
Figure 3. The microcatheter is completely inserted in one half circumference of the Schlemm canal.
Since transitioning to the OMNI device from VISCO 360 2.5 years ago, I have already performed 24 procedures. I have been extremely impressed with early results, which I share below.
LEARNING CURVE AND POINTERS
The learning curve for the average surgeon is quite short. The only difficulties, at the beginning, are related to the use of the gonio lens, which the surgeon should quickly get used to, and the opening of the Schlemm canal to introduce the tip of the device. After a few operations, the procedure becomes easy and can usually be completed in less than 10 minutes.
Ab interno canaloplasty can be successfully combined with phacoemulsification4,5 and other MIGS procedures.6 The mid-term results with VISCO 360/OMNI canaloplasty are encouraging. In the 35 standalone surgeries of this type that I have performed, all were done in pseudophakic patients. The main indications were primary open-angle glaucoma and pseudoexfoliation glaucoma that was insufficiently controlled with medical therapy. Most patients had mild to moderate glaucoma. I have also performed the procedure in eyes with a previous failed trabeculectomy or deep sclerectomy.
The OMNI device can be used not only to dilate the Schemm canal but also to perform an ab interno titratable trabeculotomy. This is achieved by pulling the microcatheter through the TM to unroof the tissue, creating a direct path for the outflow of aqueous through the Schlemm canal and distal collector channels (Figure 4).
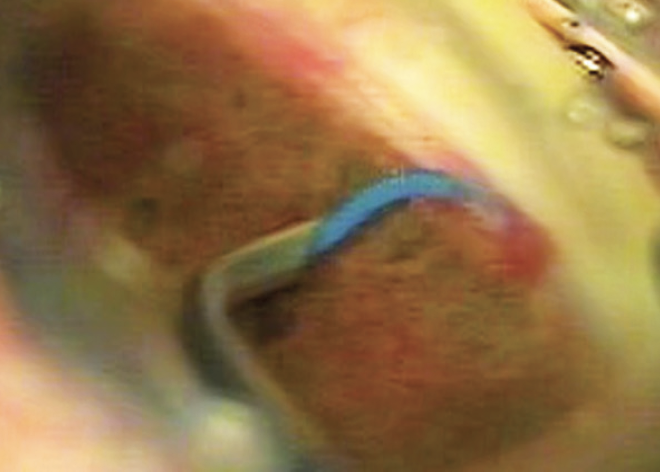
Figure 4. The microcatheter is removed, producing an ab-interno trabeculotomy.
The trabeculotomy can be performed in both hemispheres, opening the Schlemm canal for 360º, or can be titrated to one (180°) or even a portion of one hemisphere (~90°). An important benefit of the OMNI Surgical System is that the amount of trabeculotomy performed can be titrated to match the surgical plan for patients. Slight reflux in the anterior chamber is usually observed after this maneuver and can sometimes disturb visibility of the angle, especially if both sections of the canal have been opened. For this reason, I prefer to perform trabeculotomy in one hemisphere of the canal only.
I have also performed the procedure in eyes with a previous failed trabeculectomy or deep sclerectomy. The mean preoperative IOP of all operated cases was 24.8 ±5.6 mm Hg (range, 16-40 mm Hg) with an average of 3.1 medications. The IOP values after 6 and 12 months were 17.3 ±5.0 mm Hg (range, 7-34 mm Hg) and 17.2 ±3.6 mm Hg (range, 14-26 mm Hg), respectively, with an average of 1.4 and 1.7 medications, respectively. Mean IOP reduction after 6 and 12 months was 7.5 mm Hg (30.2%) and 7.6 mm Hg (30.6%), respectively. Seven eyes required a reoperation over time because of insufficiently controlled IOP.
An additional benefit of ab interno canaloplasty is that it could likely be repeatable if the TM is still intact. If a patient does not achieve the target IOP or medication reduction, a repeat procedure could be attempted. Of course, canaloplasty is not possible when an ab interno trabeculotomy was combined with canaloplasty. Even in that case, however, using the OMNI preserves the ability to move to more aggressive procedures such as deep sclerectomy or, in rare cases, a trabeculectomy.
CONCLUSION
I have had a positive early experience with the standalone ab-interno canaloplasty and partial trabeculotomy procedure with the OMNI device. Careful patient selection, however, is crucial for the success of this safe, effective, and efficient procedure.
1. Körber N. Canaloplasty ab interno – a minimally invasive alternative. Klin Monbl Augenheilkd. 2017;234(8):991-995.
2. Gallardo MJ, Supnet RA, Ahmed IIK. Viscodilation of Schlemm’s canal for the reduction of IOP via an ab-interno approach. Clin Ophthalmol. 2018;12:2149-2155.
3. Ondrejka S, Körber N. 360° ab-interno Schlemm’s canal viscodilation in primary open-angle glaucoma. Clin Ophthalmol. 2019;13:1235-1246.
4. Tracer N, Dickerson JE Jr, Radcliffe NM. Circumferential viscodilation ab interno combined with phacoemulsification for treatment of open-angle glaucoma: 12-month outcomes. Clin Ophthalmol. 2020;14:1357-1364.
5. Brown RH, Tsegaw S, Dhamdhere K, Lynch MG. Viscodilation of Schlemm canal and trabeculotomy combined with cataract surgery for reducing intraocular pressure in open-angle glaucoma. J Cataract Refract Surg. 2020;46(4):644-645.
6. Heersink M, Dovich JA. Ab interno canaloplasty combined with trabecular bypass stenting in eyes with primary open-angle glaucoma. Clin Ophthalmol. 2019;13:1533-1542.
