
In just a few short years, Small Incision Lenticule Extraction has come full circle, from a surgical novelty practiced by a minority of surgeons to a mainstream technique adopted by the wider ophthalmic profession. I started performing SMILE in 2014, when I was the head of the refractive department at the University in Munich. However, it was only when I switched to private practice that I started to perform a much higher volume of Small Incision Lenticule Extractions. After the initial learning curve, I became more familiar with the nuances of the procedure and was in a position to truly offer my patients the most common kinds of laser vision correction: surface ablation, LASIK, and SMILE.
A lot has been written and said about the learning curve with SMILE. Speaking to colleagues and reading the scientific literature, I learned that the learning curve is different for SMILE than it is for LASIK and surface ablation techniques. At the university clinic, I performed keratoplasty procedures, including Descemet membrane endothelial keratoplasty (DMEK). My experience with corneal surgery helped a lot when I first started with SMILE, and it helped to shorten the learning curve. I was also fortunate to be able to call on the expertise of experienced colleagues, who could advise on pitfalls to avoid and also share useful techniques to ensure optimal results.
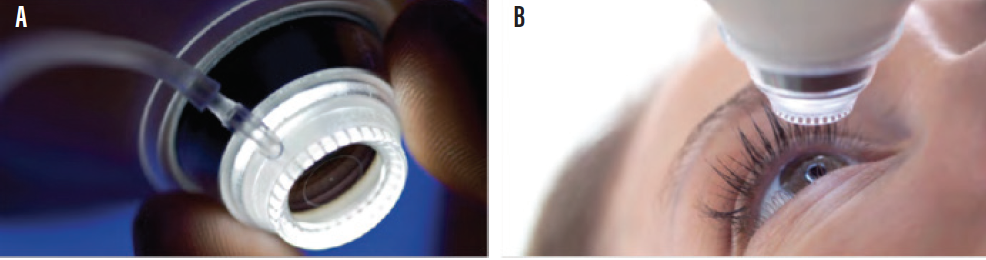
Figure 1. The contact glass on the VisuMax (A) is designed to fit the anatomy of the eye (B). As a result, the cornea largely retains its natural physiological shape.
COMPLICATIONS AND BENEFITS
Taking into account surgical experience, all types of laser vision correction surgery are safe, as long as the indications and contraindications of each procedure are respected. Nevertheless, there are key differences between the procedures.
From my perspective, one of the principal benefits of SMILE is that it induces less dry eye than LASIK.1,2 Many patients have some degree of dry eye after refractive surgery, which usually resolves spontaneously and at varying times depending on the individual patient and the chosen procedure. For patients aged around 40 who present with dry eye, I recommend SMILE rather than LASIK if there are no other contraindications.
I try not to systemically recommend the same procedure for every patient. Rather, I spend a lot of time getting to know each patient, devising an individualized treatment plan and taking in account his or her particular needs and expectations. It might be surface ablation, or there may be some reason why LASIK is not suitable.
From my perspective, there is not one best technique for every situation, and there is no “one size fits all” approach to refractive surgery. We have more than 30 years of experience with LASIK and PRK, and both continue to be excellent options depending on the specific needs of our patients and their anatomical characteristics.
For younger patients with myopia, low astigmatism, and a normal cornea, I usually propose SMILE; for a patient with high astigmatism or irregular corneal topography, femto-LASIK would probably be a better option. The bottom line is that refractive surgeons are in a position to provide a truly customized approach with the excellent surgical techniques available today.
In terms of contraindications for SMILE, it is important to closely assess the anatomical structure of the cornea. If the patient has a steep but otherwise healthy cornea, there is a slight risk that the surgeon may run into problems with the laser cone during the docking phase of the procedure (Figure 1). In this instance, the patient should be warned of the possibility that the procedure must be aborted and a surface ablation performed a week later. If he or she accepts that risk, then I will proceed with SMILE. When the patient has given consent and has been fully informed, he or she can more readily accept a conversion to surface ablation if required.
CHANGING LASER VISION CORRECTION MARKET
The demand for refractive surgery has been fairly stable over the past decade. In Germany, an estimated 100,000 to 110,000 eyes undergo refractive surgery every year.3 Like a lot of other European countries, however, the laser vision correction market in Germany is currently undergoing a slow but progressive transformation due to demographic factors and the availability of new technology and surgical techniques. First, the market for presbyopic correction is growing in Germany. This is no surprise: Of the total German population (approximately 80 million), 24.1 million are between the ages of 40 and 59, and this the largest age group in Germany. Although the rise in myopia in Germany aligns with global trends in developed countries, the change in the population profile means that fewer young people are seeking laser vision correction to treat their refractive errors. The result is that a lot of clinics that offer LASIK are experiencing less demand because of the population change.
By contrast, we are seeing strong growth and demand for minimally invasive surgery, and more patients are coming to the clinic asking for it. An estimated 60,000 eyes are treated by femtosecond laser annually, and SMILE’s current market share is about 33% and increasing every year. Our patients today are better informed. They understand the principle behind lenticule removal (Figure 2) and the potential benefits that minimally invasive surgery offers. They like the idea of not having a flap with less risk for dry eye. It seems probable that SMILE will gain further market share once treatments for high astigmatism and hyperopia become available in the near future.
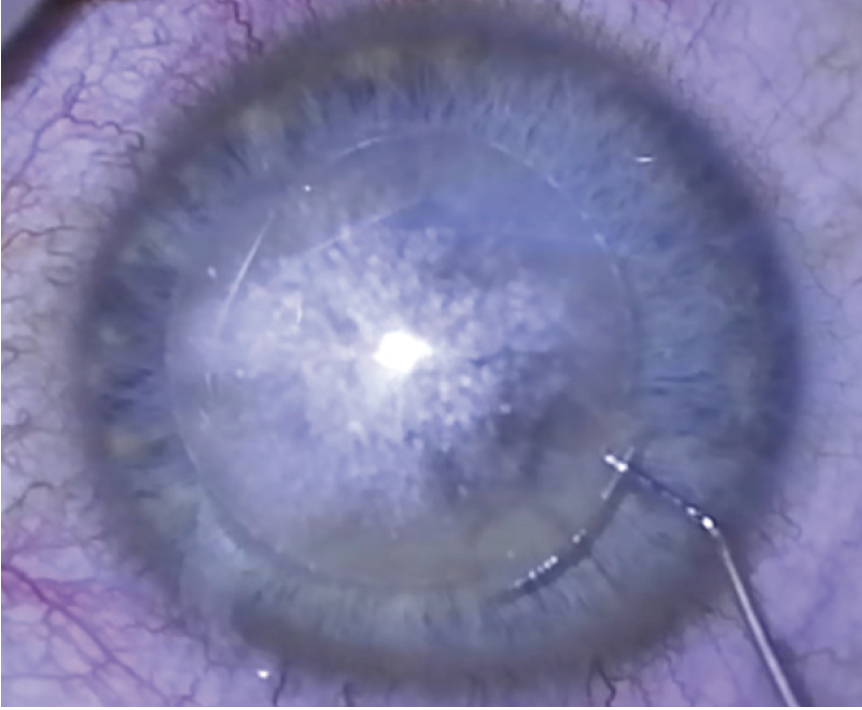
Figure 2. During SMILE, the lenticule will be removed through a small incision.
POTENTIAL BARRIERS
What holds patients back from having refractive surgery? Financial considerations play a role. SMILE is considerably more expensive than LASIK, but it is not the primary obstacle in my view. It would be nice to be able to offer patients what is best for them, irrespective of the technique or the price, but that is not always possible. However, it is more transparent for patients, as they know that they are given advice purely on the medical merits of the case rather than any financial considerations.
There is also a psychological issue. Patients are aware that laser vision correction is surgery, and they can be afraid of complications. It is important that they have trust in their doctor, the technology, and the postoperative care team.
My feeling is that, in the future, we will see less demand for LASIK and surface ablation procedures as the demand for SMILE continues to grow. But LASIK, of course, will not disappear any time soon. I think there will be room for flap-based procedures for the foreseeable future, particularly for hyperopes who currently have less treatment options compared to myopes. The most important thing is to be able to offer our patients a range of safe, effective, and reliable procedures that deliver excellent quantity and quality of vision.
For the growing market of presbyopic patients, monovision can be a safe and effective option. If the patient is older than 50 years of age and has some issues with monovision, however, then an IOL procedure would be my first choice. The same applies to high myopes who tend to develop a cataract earlier. Once the retina is okay and there are no other contraindications, I would usually opt for an intraocular procedure for them as well.
LEGACY OF laser vision correction
A very important point to bear in mind is that around 2% of patients currently presenting for intraocular surgery have undergone laser vision correction in the past—and the number is growing. Some patients, particularly hyperopes, have had high ametropic corrections years ago, and some of them had subsequent enhancements. The result is that we are often faced with a multifocal cornea, so implanting a multifocal IOL in these patients is not a viable treatment strategy because it generates optical phenomena and compromises quality of vision.
For those who have undergone surface ablation, it depends on the cornea: Is there presence of asphericity, higher-order aberrations, or irregular astigmatism, for instance? A multifocal IOL may still be an option if all is normal with the eye, but the calculation of IOL power is also less predictable for these complex eyes.
We need to engage with patients when they first come to our clinics requesting a refractive procedure, and we must explain that performing a hyperopic ablation might have implications if they opt for a multifocal lens in 10 or 15 years’ time. We see a lot of patients after hyperopic treatment who can no longer have a multifocal lens and who might have made a different choice had they known about this possibility 5 or 10 years earlier. The long-term picture of ocular health should be in the forefront of the surgeon’s mind when discussing treatment options with patients.
CONCLUSION
The laser vision correction market in Germany is changing due to demographic factors and the advent of new treatment options for patients. SMILE has transformed our refractive surgery practice because it delivers excellent visual outcomes, and it is well placed to capitalize on the growing demand for minimally invasive surgery.
Explore more and get in contact!
1. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C. Dry eye disease after refractive surgery: Comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122:669-676.
2. Bingjie W, Naidu RK, Chu R, Dai J, Qu X, Zhou H. Dry eye disease following refractive surgery: A 12-month follow-up of SMILE versus FS-LASIK in high myopia. J Ophthalmol. 2015. https://doi.org/10.1155/2015/132417.
3. Internal data on file, Carl Zeiss Meditec AG.

