
With growing popularity worldwide and a robust body of evidence in the scientific literature,1-4 Small Incision Lenticule Extraction has firmly established its credentials as a safe, accurate, and efficacious refractive surgery procedure (Figure 1). I was fortunate to be one of the early adopters of the technology, and I performed my first procedure with SMILE using the VisuMax femtosecond laser (Carl Zeiss Meditec) in 2013.
My enthusiasm to move to this new approach to refractive surgery seemed like a natural evolution. I was convinced by the early results of and from conversations with Walter Sekundo, MD, PhD; Rupal Shah, MD; and other SMILE pioneers that this approach represented the future of minimally invasive refractive surgery. I have no cause to regret my decision: My practice volume multiplied by a factor of 4, and SMILE has completely replaced femtosecond LASIK with the exception of the procedures I perform in hyperopes and presbyopes.
At the beginning of our clinical experience with SMILE, we quickly realized that postoperative visual recovery took slightly longer than with LASIK in order for patients to attain 20/10 vision. It was also clear that this experience was not confined to our practice alone.5,6 At that time in 2013, my approach to dealing with the delay in visual recovery was to tell patients about it upfront. I perform refractive surgery on Fridays. On the day of surgery, I would tell patients that when I would see them on their postoperative day 1 follow-up visit that their vision would not be perfect, but close to it. After relaxing on Sunday, they could then anticipate returning to their normal activities on Monday with full visual recovery.
FOCUS ON ENERGY settings
Although delayed visual recovery was a relatively minor drawback when weighed alongside the benefits of the procedure, including that it is a minimally invasive surgery and that there is no flap or flap-related complications, less dry eye than with other laser vision correction procedures, and excellent outcomes, it still merited further investigation in an effort to establish the root cause.
Given the known importance of laser energy settings for the surface regularity of the human corneal lenticule and posterior stroma, it was surmised that reducing the levels of femtosecond laser energy into the eye might have a positive impact on visual recovery in the immediate postoperative period.7
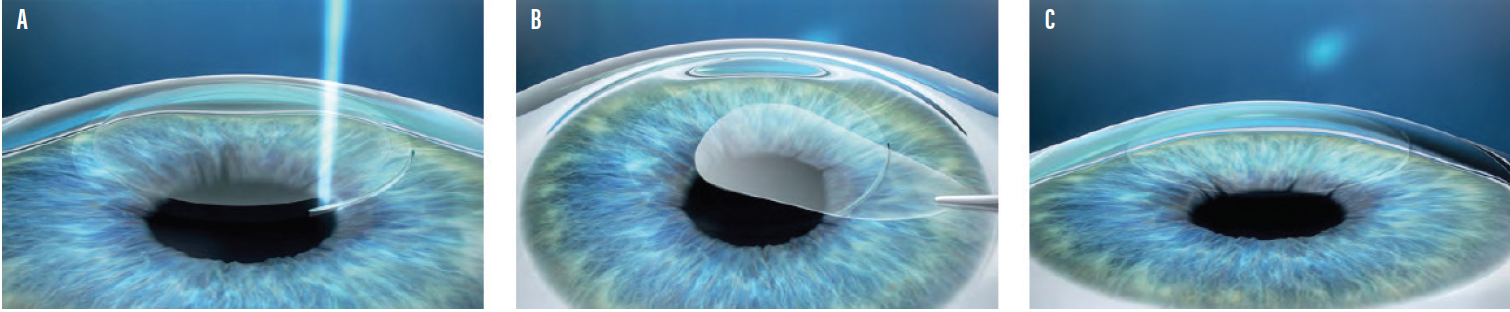
Figure 1. The three steps of Small Incision Lenticule Extraction: The creation of a refractive lenticule and a small incision in the intact cornea (A). The lenticule is removed through the small incision (B). Once the lenticule is removed, the corneal shape is altered, thereby achieving the desired refractive correction (C).
The concept of energy optimization is principally to balance the effects of femtosecond pulse energy (measured in nJ), tracking distance and spot separation to make sure the energy delivered into the eye is not too high or too concentrated in one area. If the energy is too high, an opaque bubble layer (OBL) will be created. Although OBL is not thought to affect clinical outcomes in the longer term, it can lead to delayed visual recovery or interfere with the penetration of femtosecond laser pulses. This can result in difficult tissue dissection and residual marginal lenticule.8 It can also make it difficult to visualize and perform lenticule dissection. By contrast, if the energy levels are too low during SMILE, it can result in increased adhesions and become extremely difficult to separate the tissue in order to remove the lenticule. When this happens, the only option for the surgeon may be to abort SMILE entirely.
TWEAKING THE SETTINGS
SMILE performed on the VisuMax laser platform has three preset modes of treatment: (1) standard, (2) fast, and (3) expert. The standard mode is the default laser parameters set by the manufacturers, and the expert mode has modifiable laser settings that can be optimized by the surgeon according to his or her preferences and clinical experience. The fast mode, which consists of preset laser parameters customized according to region, may be altered only by ZEISS specialists.
In our experience with SMILE over many years, anything above an average energy offset of 35 and a pulse energy of 175 nJ is considered too high. A suboptimal energy setting is anything less than 20 offset and a pulse energy of 100 nJ, which is the plasma threshold level. The ideal energy level is located somewhere between 20 and 30 offset and 100 to 150 nJ and will vary slightly from laser to laser.
My advice for a surgeon just starting with SMILE is to follow the ZEISS SMILE onboarding process. A regional clinical application specialist will help to find the optimal settings for the laser. In general, it is preferable to use the lowest possible energy levels; however, if the surgeon notices black spots appearing on the cornea, he or she should not lower the energy settings any further. These spots are thought to form through the adherence of water droplets or meibomian secretions to the interface between the suction cone and cornea. They may locally block photodisruption and must be manually separated during lenticule dissection, so it is best to keep the energy setting sufficiently high to preclude their appearance.
In summary, the key to successful outcomes is to modulate the energy settings until a “sweet spot” of energy levels is obtained. This energy level is sufficiently high to ensure safe and easy tissue dissection yet low enough to avoid impacting the postoperative visual recovery.
BALANCING ACT
Finding the right energy level is a delicate balancing act, but with enough practice and by drawing on the experience of ZEISS representatives and other surgeons as required, it should be perfectly attainable for all refractive surgeons who opt to convert to SMILE. One particular sign to watch for when experimenting with settings is gas bubbles escaping from the incision site as it is opened. This is usually a positive sign that the sweet spot for energy optimization has been reached and smooth lenticule extraction can be assured without any negative impact on immediate postoperative visual recovery.
Since we optimized our energy settings, about 99% of our patients now attain binocular UCVA of 20/20 on postoperative day 1. It is no longer necessary to warn patients in advance of potential issues with their visual recovery, and most can drive and perform their usual activities within 24 hours of surgery.
Our own experience with lower energy settings has also been validated in some recent clinical studies. Donate and Thaëron, for instance, conducted a study assessing early visual and optical quality recovery after SMILE using laser energy level settings close to the plasma threshold. They found that this approach had minimal effect on ocular scatter, and it achieved better and faster visual recovery in patients with moderate myopia.9 In another study by Ji et al, different energy levels in lenticule extraction were compared. The authors concluded that it may be advisable to reduce femtosecond laser energy to less than 115 nJ at a spot separation of 4.5 μm in order to achieve better visual outcomes with faster recovery after SMILE.10
SPOT SETTINGS AND OTHER PEARLS
One other important strategy to improve laser settings and enhance outcomes is to use differential spot spacing. Since collagen fibers are thinner and more compact in the upper corneal stroma and thicker and more dispersed in the lower stroma, it is advisable to set the spot distance slightly wider (4.5 μm) for the cap cut and slightly narrower (4.2 μm) for the lenticule cut. This makes a total energy output of 6.9 μm for the cap cut and 7.9 μm for the lenticule cut.
Surgeons who are already comfortable performing SMILE might gain additional benefit by using the “no dissection” technique for lenticule removal.11 This technique was first described by Sri Ganesh, MD. After docking and laser delivery, a microforceps is used to grasp the lenticule and gently peel it from the underlying stromal bed, without performing any dissection of the upper and lower planes of the lenticule. For this technique, which Dr. Ganesh calls “lenticuloschisis,” a minimum lenticule thickness of 25 to 30 µm is required. Initial results suggest lenticuloschisis produces a clearer and smoother interface postoperatively, which, apart from the new surgical technique, is also caused by optimizing energy levels below 115 nJ.
Another simple trick I like to teach beginners is not to hold their instruments too tightly in order to ensure a smoother dissection. The use of the Breyer-Pfäffl SMILE dissector that I developed in association with Geuder further improves the lenticule dissection, especially in more complex cases.
MAXIMIZE YOUR SETTINGS
Energy level
- The key to successful outcomes is to modulate the energy settings until a “sweet spot” of energy levels is obtained.
- An energy level that is too high is anything above an average energy offset of 35 and a pulse energy of 175 nJ.
- A suboptimal energy setting is anything less than 20 offset and a pulse energy of 100 nJ, which is the plasma threshold level.
- The ideal energy level is located somewhere between 20 and 30 offset and 100 to 150 nJ and will vary slightly from laser to laser.
Spot Spacing
- It is advisable to set the spot distance slightly wider (4.5 μm) for the cap cut and slightly narrower (4.2 μm) for the lenticule cut.
- This makes a total energy output of 6.9 μm for the cap cut and 7.9 μm for the lenticule cut.
CONCLUSION
Optimizing energy settings with the VisuMax femtosecond laser helps to achieve a uniform smooth bubble layer with minimal adhesions and smoother lenticule removal. For the patient, optimal energy into the eye equates to faster visual recovery in the immediate postoperative period.
Based on the experience of hundreds of happy patients at our clinic, I believe SMILE currently offers the best and safest method to correct myopia and myopic astigmatism in suitable candidates. Its safety, effectiveness, predictability, and long-term results are scientifically well proven.
Explore more and get in contact!
1. Hansen RS, Lyhne N, Grauslund J, Vestergaard AH. Small-incision lenticule extraction (SMILE): outcomes of 722 eyes treated for myopia and myopic astigmatism. Graefes Arch Clin Exp Ophthalmol. 2016;254: 399-405.
2. Pedersen IB, Ivarsen A, Hjortdal J. Three-year results of small incision lenticule extraction for high myopia: refractive outcomes and aberrations. J Refract Surg. 2015;31:719-724.
3. Blum M, Taubig K, Gruhn C, Sekundo W, Kunert KS. Five-year results of small incision lenticule extraction (ReLEx SMILE). Br J Ophthalmol. 2016;100:1192-1195.
4. Han T, Zheng K, Chen Y, Gao Y, He L, Zhou X. Four-year observation of predictability and stability of small incision lenticule extraction. BMC Ophthalmol. 2016;16:149.
5. Kamiya K, Igarashi A, Ishii R, Sato N, Nishimoto H, Shimizu K. Early clinical outcomes, including efficacy and endothelial cell loss, of refractive lenticule extraction using a 500 kHz femtosecond laser to correct myopia. J Cataract Refract Surg. 2012;38:1996-2002.
6. Shah R, Shah S. Effect of scanning patterns on the results of femtosecond laser lenticule extraction refractive surgery. J Cataract Refract Surg. 2011;37:1636-1647.
7. Kunert KS, Blum M, Duncker GI, Sietmann R, Heichel J. Surface quality of human corneal lenticules after femtosecond laser surgery for myopia comparing different laser parameters. Graefes Arch Clin Exp Ophthalmol. 2011;249:1417-1424.
8. Wang Y, Zhao K. Refractive Surgery with Femtosecond Laser. Beijing: People’s Medical Publishing House. 2014:116-118.
9. Donate D, Thaëron R. Lower energy levels improve visual recovery in small incision lenticule extraction (SMILE). J Refract Surg. 2016;32:636-642.
10. Ji Y W. et al. Effect of lowering laser energy on the surface roughness of human corneal lenticules in SMILE. J Refract Surgery. 2017;33(9):617-624 .
11. Ganesh S, Brar S. Lenticuloschisis: A “no dissection” technique for lenticule extraction in small incision lenticule extraction. J Refract Surgery. 2017;33:563-566.

