

Laser cataract surgery, as performed with a femtosecond laser, has been around since 2009,1 and it has by now become routine in many eye clinics. Due to high cost and logistic complexity, however, laser cataract surgery has penetrated the cataract market only to a certain extent.2-4 In the meantime, the technology of the lasers continues to evolve.
A new laser, the Femtomatrix (Keranova; Figure 1), features a robotic arm and several unique technical innovations that may serve to put this laser ahead of all others currently available. A video demonstrating cataract surgery with the Femtomatrix laser can be seen here: https://f.io/syQE0GCJ. This article describes the technology behind the laser and our first clinical experience with its use.

Figure 1. The Femtomatrix laser.
ROBOTIC ARM
The Femtomatrix laser incorporates a robotic arm that simplifies the eye-docking procedure and allows the laser portion of the laser cataract surgery procedure to be performed in the OR rather than in a separate laser room. The arm is designed for optimal efficacy, safety, and comfort of the docking procedure. It moves automatically into the surgical space for laser treatment close to the patient’s eye, and at the end of the laser procedure it leaves its position so that the surgeon can immediately use the microscope to continue the intraocular portion of the procedure without moving him- or herself or the patient.
The robotic arm of Keranova’s laser device features six axis segments that move with adjustable speed according to the distance from the patient and with impressive precision of position, to an accuracy of 50 µm.
The robotic docking mechanism can couple the patient’s eye with the laser on its own, with limited or no assistance from the surgeon. Before docking of the robotic arm, the surgeon attaches an aspirating cone to the patient’s anesthetized eye, and the robotic arm brings the laser head close to the cone. The eye is connected to the laser through the aspirating cone with a flat glass plate. A liquid then automatically fills the space between the glass and the cornea.
ENERGY management
As soon as the eye is connected, real-time OCT displays the anterior segment intraocular structures. After ocular landmarks are verified, the Femtomatrix laser sends a sample laser beam into different areas of the crystalline lens (Figure 2A) to determine the proper energy needed for lens fragmentation in each area (Figure 2B).
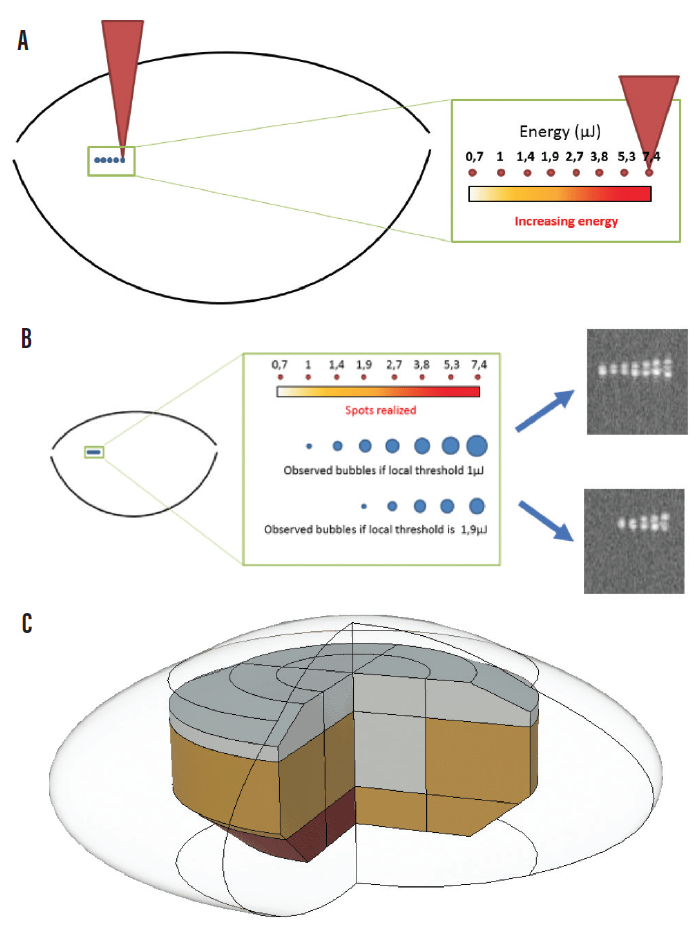
Figure 2. TSS technology step 1: Laser energy is successively increased in one tested spot in a given lens area until a bubble is detected (A). TSS technology step 2: OCT detects the bubbles created by the sample laser beam, and the energy threshold for fragmentation is determined (B). TSS technology step 3: Replication of steps 1 and 2 in 24 locations within the lens results in creation of a 3D threshold map that is used to guide efficient lens photoemulsification (C).
This three-step OCT-guided Threshold Scanning System (TSS) process is used to detect the varied tissue photodisruption thresholds throughout the lens. This capability not only lowers the laser energy delivered inside the eye, but it also avoids bubble creation in the lens and anterior chamber caused by excess laser energy. TSS takes only a few seconds during the treatment planning phase of the Femtomatrix cataract procedure.
After the TSS analysis, based on a 3D threshold map (Figure 2C), the Femtomatrix laser system can then apply the optimal amount of energy and number of laser spots into different parts of the lens across the range of cataract grades. Through this process, the laser achieves the most efficient photoemulsification procedure, avoiding creation of too much gas inside the capsular bag while ensuring complete laser dissection of the tissue throughout the lens volume.
FASTER CUTTING
Another principal innovation of the Femtomatrix laser is laser spot multiplication by a phase mask. The laser beam is directed to a dynamic phase mask that modifies the laser wavefront to create multiple laser spots at the target tissue (Figure 3). The shape of the phase mask can change in a matter of milliseconds, allowing the laser to dynamically change the number of spots and the distance between them, the geometry of the matrix obtained, the energy of each spot, and the position of the spots in three dimensions.
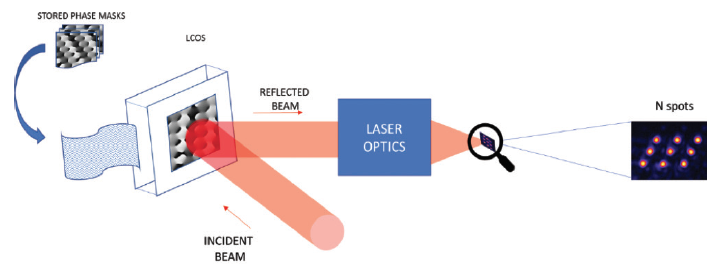
Figure 3. A phase mask is used to achieve laser spot multiplication.
The laser can create six or even more spots in the lens or cornea at the same time, cutting the eye tissue up to 20 times faster than current femtosecond lasers. What does this mean in eye surgery? In cataract surgery, the Femtomatrix laser can cut a human cataractous lens into 20,000 small cubes in a 0.2-mm3 volume in 20 sec (Figure 4). Such cubes can then be aspirated without any use of ultrasound in most cases. In refractive surgery, the Femtomatrix laser could create a LASIK flap in only 0.5 sec—considerably less time than needed by other current flap-creation technologies.
Figure 4. The first human lens fragmented into 20,000 cubes within a volume of 0.2-mm3 using the Femtomatrix laser.
Keranova has also managed another innovation: to transmit the femtosecond laser beam via optical fiber. This is obviously an important technical advantage over the complex optical paths used by other femtosecond lasers.
CLINICAL EXPERIENCE
We have performed the world’s first cataract surgeries assisted by the Keranova Femtomatrix laser. The laser was used to perform capsulotomy and lens fragmentation in 27 eyes of 27 patients with cataract grades 1 to 5. In all cases, docking was uneventful and a complete circular capsulotomy was achieved. Fragmentation was also achieved in all cases, and there was no need to use any ultrasound for lens material emulsification in 25 cases, which means that 93% of cataracts were photoemulsified with zero phaco energy. All 27 surgeries in which the laser was used for capsulotomy and lens fragmentation were uneventful (unpublished data).
At the time of this publication, all eyes examined at 1-month follow-up had clear corneas and achieved best corrected distance visual acuity of 0.0 logMAR. Final compilation of the feasibility study results are under way, and we look forward to presenting and publishing the data later this year.
CONCLUSION
The first short-term experience with the robotic arm Femtomatrix laser for laser cataract surgery has been promising. Obviously, further clinical evaluation in a larger number of surgeries with longer follow-up will be needed.
Additional applications of the Femtomatrix laser technology in eye surgery will follow. In the pipeline are use of the laser for refractive surgery procedures such as LASIK, intrastromal lenticule extraction, and creation of pockets for biocompatible presbyopic inlays. Further down the pike will be corneal applications such as penetrating or lamellar keratoplasty, and the creation of tunnels for intrastromal corneal ring segment procedures.
Is this device the next significant step toward automation of cataract surgery? Time will tell, as we are looking forward to continuous improvement of tools to serve our cataract practice.
1. Nagy Z, Takacs A, Filkorn T, Sarayba M. Initial clinical evaluation of an intraocular femtosecond laser in cataract surgery. J Refract Surg. 2009;25(12):1053-1060.
2. Roberts HW, Wagh VK, Mullens IJM, Borsci S, Ni MZ, O’Brart DPS. Evaluation of a hub-and-spoke model for the delivery of femtosecond laser-assisted cataract surgery within the context of a large randomised controlled trial. Br J Ophthalmol. 2018;102(11):1556-1563.
3. Quinones A, Gleitsmann K, Freeman M, et al. Benefits and harms of femtosecond laser assisted cataract surgery: a systematic review. US Department of Veterans Affairs. Evidence-Based Synthesis Program. Washington, DC; 2013.
4. Song C, Baharozian CJ, Hatch KM, Talamo JH. Assessment of surgeon experience with femtosecond laser-assisted cataract surgery. Clin Ophthalmol. 2018;12:1373-1377.
